الأساس العلمي لعقار Arthrosamid® (iPAAG)
علاج جديد للبالغين المصابين بالفُصال العظمي في الركبة
Arthrosamid® هو جل شفاف مسترطب غير قابل للامتصاص وغير قابل للتحلل الحيوي وقابل للحقن، ويتكون في الأساس من البولي أكريلاميد المترابط بقوة وغير القابل للتحلل الحيوي بنسبة (2.5٪) ومياه مرتبطة به غير مولّدة للحرارة بنسبة (97.5٪)
يأتي Arthrosamid® في صورة محقنة معقَّمة مملوءة مسبقًا للاستخدام الفردي سعة 1 مل، ومغلقة بتركيبة قفل لور وغطاء للطرف. وهي مخصصة للحقن داخل المفصل في مفصل الركبة بإبرة معقَّمة عيار 21 × 2 بوصة (0.8 × 50 ملم).
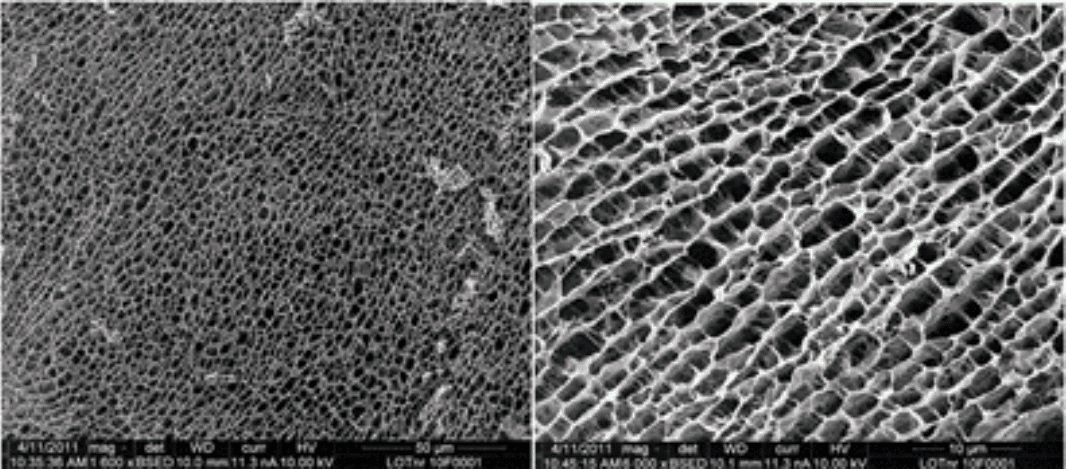
يوضح الشكل 1 الهيكل ثلاثي الأبعاد لجل مائي من البولي أكريلاميد. ويوفر هيكل قرص العسل المنتظم المُحكَم مصفوفة لنشوب الخلايا.
الوصف الكيميائي للبولي أكريلاميد
كما أوضحنا أعلاه، يتكون الجل المائي لعقار Arthrosamid® من 2.5٪ بولي أكريلاميد ذي روابط متقاطعة جاف و97.5٪ ماء غير مولّد للحرارة. أثناء تصنيع المركب، يتبلمر N، N، الميثيلين-ثنائي-أكريلاميد مع الأكريلاميد، مما يؤدي إلى إنشاء روابط متقاطعة بين سلاسل البولي أكريلاميد.
يتم تصنيع مركب الجل المائي من البولي أكريلاميد ذا الروابط المتقاطعة في عملية بلمرة يتم فيها ربط الوحدات المتكررة من الأكريلاميد في تفاعل متسلسل.
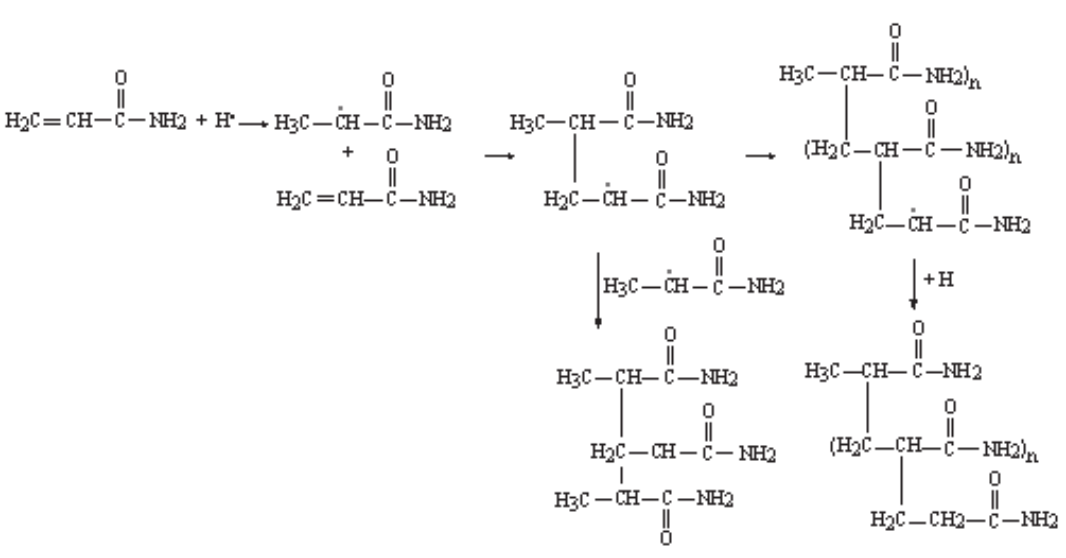
يتضمن التفاعل المتسلسل مبدأ بادئ الأكسدة والاختزال، حيث يولّد بادئ كبريتات الأمونيوم (AMPS) جذرًا حرًا يضيف مونومر أكريلاميد عن طريق الحصول على إلكترون من الرابطة المزدوجة في الأكريلاميد، وبالتالي تكوين رابطة كربون-كربون مفردة مع مادة الأكريلاميد. وهذا يترك إلكترونًا غير مشترك لإضافة مزيد من مونومرات الأكريلاميد على النحو الموضح في الشكل 2 على اليمين.
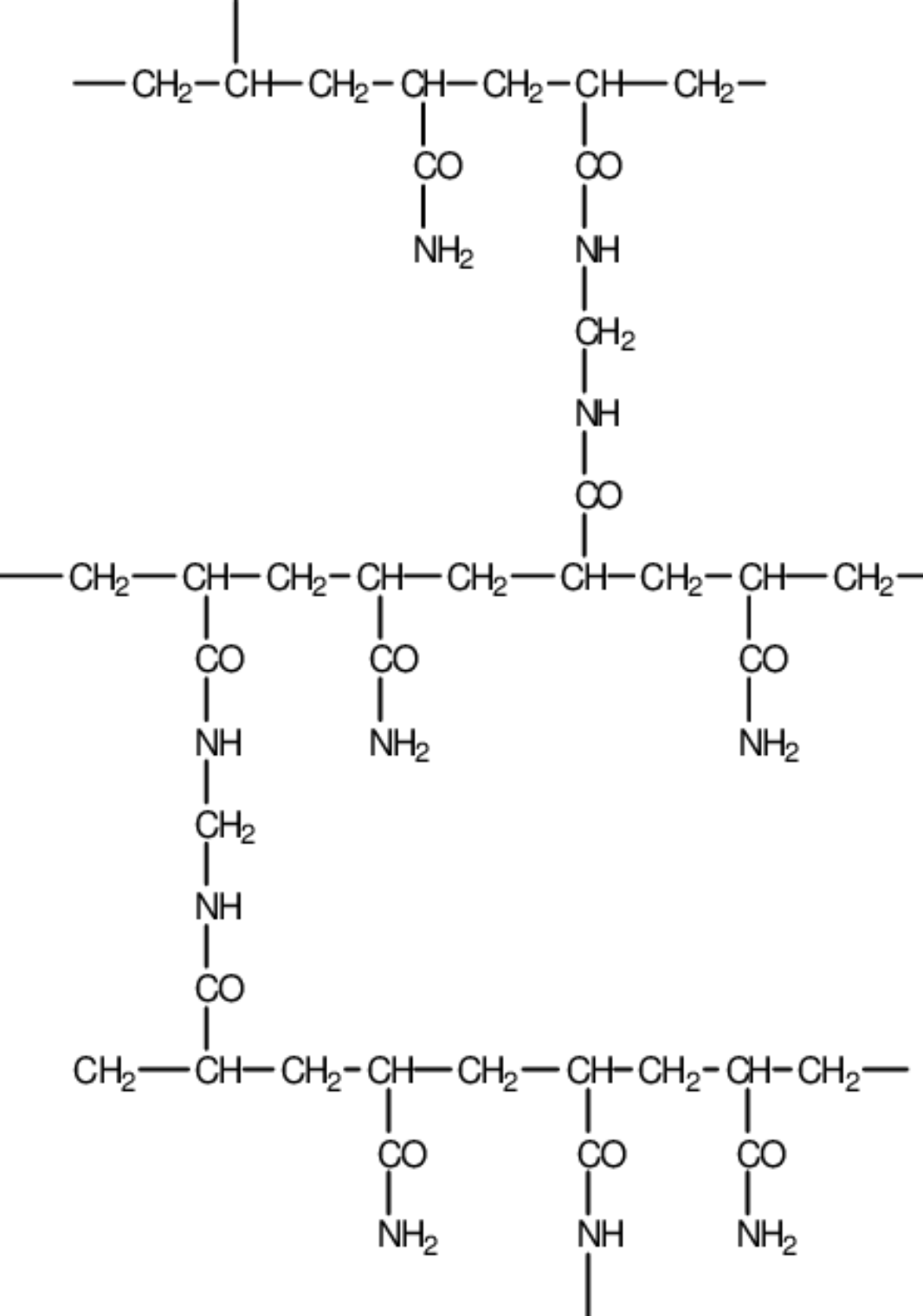
سيحدث تفرع الأساس الخطي لرابطة كربون-كربون للبولي أكريلاميد بسبب وجود عامل ربط متقاطع، N، N، الميثيلين-ثنائي-أكريلاميد مونومر (MBAM) على النحو الموضح في الشكل 3.
بعد تفرع سلاسل بولي أكريلاميد الأساسية، يتم تشكيل شبكة ثلاثية الأبعاد من بولي أكريلاميد ذي الروابط المتقاطعة، بدلاً من سلاسل خطية غير متصلة من البولي أكريلاميد.
مواد Arthrosamid® والتوافق الحيوي
لا يشتمل عقار Arthrosamid® على مادة طبية أو أنسجة أو منتجات دموية.
المواد المستخدمة في Arthrosamid® هي المذكورة فيما يلي (الجدول 2).
جزء الجهاز |
المادة |
ملامسة الجسم |
|
|---|---|---|---|
جل |
جل مائي يتكون من حوالي 2.5٪ بولي أكريلاميد ذي روابط متقاطعة و97.5٪ ماء غير مولّد للحرارة |
مفصل الركبة |
|
محقنة |
أنبوب |
بولي بروبلين |
الجلد* |
مكبس |
بولي كربونات |
الجلد* |
|
سدادة مطاطية |
مطاط سيليكون |
الجلد* |
|
مزلّق |
زيت سيليكون |
الجلد* |
|
غطاء الطرف |
بولي بروبلين |
الجلد* |
|
الجدول 2: مواد الجهاز. *يجب أن يتعامل المستخدم مع المحقنة وهو مرتدٍ قفازًا واقيًا. وبالتالي، ينبغي عادةً ألا يُلامس المريض والمستخدم المحقنة. كما أن السدادة المطاطية والمزلّق غير مكشوفين، وبالتالي فإن خطر ملامستهما يكون أقل حتى من أجزاء المحقنة المكشوفة.
تم إجراء اختبار التوافق الحيوي وفقًا للمعيار ISO 10993-1 لمنتجات Contura الحالية من الجل المائي، ويرد فيما يلي ملخص الاختبارات (الجدول 3) التي تعتبر ذات صلة بعقار Arthrosamid® وذلك إلى جانب وصفها بالتفصيل في تقرير التقييم البيولوجي (BER) - Arthrosamid®.
نقطة نهاية التقييم البيولوجي |
المرجع القياسي |
الاختبار ورقمه |
تاريخ التقرير |
النتيجة |
|---|---|---|---|---|
السُميّة الخلوية |
ISO 10993-5:2009 USP 29 |
الجل المائي ب: اختبار السُميّة الخلوية في المختبر رقم 16/368-030C |
2017 |
اجتاز الاختبار |
التحسيس |
ISO 10993-10: 2010 |
تقييم فرط الحساسية التلامسية في مقايسة العقدة الليمفاوية المحلية لخنزير غينيا (اختبار التعظيم) في الفئران رقم 517557 |
2017 |
اجتاز الاختبار |
الجل المائي ب: مقايسة العقدة الليمفاوية المحلية (حساسية الجلد) رقم 77691 |
2017 |
|||
التهيج أو التفاعل داخل الجلد |
ISO 10993-10: 2010 |
اختبار التفاعل داخل الجلد في الأرنب رقم 77693 |
2017 |
اجتاز الاختبار |
السُميّة الجهازية (حادة) |
ISO 10993-11: 2017 / 10993-12: 2012 USP 151 |
اختبار توليد الحرارة عبر المواد رقم APS-GZJ009-ST01 |
2018 |
اجتاز الاختبار |
السُميّة شبه المزمنة (السُميّة دون الحادة) |
ISO 10993-6:2007 |
تم فحص نقاط نهاية السُميّة الجهازية للسُميّة شبه المزمنة في دراسة الزرع في الأغنام لمدة عامين رقم 285465 |
2017 |
اجتاز الاختبار |
السُميّة الجينية |
ISO 10993-3: 2014 |
مقايسة الطفرة العكسية البكتيرية (اختبار أميس) رقم 16/368-007M |
2017 |
اجتاز الاختبار |
اختبار انحراف الكروموسومات في الثدييات في المختبر رقم 16/368-020C |
2017 |
|||
اختبار النوى الصغيرة لخلايا الدم الحمراء في الثدييات في جسم حي رقم 16/368-013E |
7 أبريل 2017 |
|||
الزرع |
ISO 10993-6:2007 |
دراسة زرع لمدة عامين في الأغنام رقم 285465 |
2017 |
اجتاز الاختبار |
الجدول 3: دراسات التوافق الحيوي (ودراسة الزرع) المُجراة على الجل المائي لشركة Contura
بناءً على الاختبارات المُجراة، يعتبر عقار Arthrosamid® متوافقًا حيويًا وملائمًا للتلامس طويل الأمد مع الجسم.
استقرار عقار Arthrosamid® ومدى عمره
جرى وصف استقرار الجل المائي من البولي أكريلاميد الذي تصنَعه شركة Contura ومناقشته على نطاق واسع في تقرير التقييم البيولوجي (BER) - Arthrosamid®، وفيما يلي (الجدول 5) ملخص لاختبارات الاستقرار التي تبحث إمكانية التحلل المائي والإجهاد التأكسدي والبدني في "الجل المائي ب". وكما هو موضح في تقرير التقييم البيولوجي، تم اختبار التحلل الإنزيمي للبولي أكريلاميد في أنظمة تخمر إنزيمية مختلفة، ولكن لم يلاحظ وجود أي تحلل.
| الحالة | الاختبار | النتيجة | مرجع الاختبار |
|---|---|---|---|
| التحلل المائي والإجهاد التأكسدي | تم احتضان عينتين متماثلتين من الجل المائي ب لمدة 24 ساعة عند 37 درجة مئوية في مذيبات غير مؤكسدة، مؤكسدة معتدلة، شديدة التأكسد منخفضة الأسموزية ومتساوية التوتر. وأجريت مقارنة بين المذيبات المحايدة المعدلة وغير المعدلة ذات الرقم الهيدروجيني 2. وتم تحليل العينات بواسطة الاستشراب السائل رفيع الإنجاز. | لم يُظهر الجل المائي ب أي ميل لتكوين أحادي الأكريلاميد تحت ظروف الاختبار الحمضية غير المؤكسدة والمؤكسدة العدوانية والمحلِّلَة للماء. | ChemPilot 2018 |
| الإجهاد البدني | إعداد تجريبي عرَّض الجل المائي لإجهاد قص ميكانيكي شديد في إجراء مزج بالسكين. | لم يؤد الإجهاد الميكانيكي الشديد إلى تحلل الجل المائي إلى مونومرات أكريلاميد. لا تُجرى تجربة الإجهاد الميكانيكي الشديد، مثل المزج بالسكين، في أثناء ظروف فسيولوجية. | Contura (011.INR.00025) |
الجدول 5: أجريت دراسات الاستقرار على الجل المائي لشركة Contura ("الجل المائي ب").
يُلاحظ أن الجل المائي من البولي أكريلاميد مستقر ولا يتحلل في ظل ظروف الاختبار.
استقرار Arthrosamid® - التنقل
جرت دراسة إمكانية انتقال الجل المائي من البولي أكريلاميد دراسة شاملة، كما هو موضح في تقرير التقييم البيولوجي وفي تقرير "تقييم إمكانية انتقال Arthrosamid® وتحلله بعد الحقن داخل المفصل". وباختصار، فيما يتعلق بالحقن داخل المفصل، فقد لوحظ أن الجسيمات الصغيرة (8 ميكرومترات أو أقل) تخضع للبلعمة وستتدفق مع السائل الزليلي من خلال الموصلات الفجوية في الظهارة الزليلية وتُوزَّع في نهاية المطاف بشكل نظامي، بينما الجزيئات الأكبر (> 8-17 ميكرومترًا) يتم تغليفها بمرور الوقت وتبقى مستقرة داخل الأنسجة الرخوة إلى أجل غير مسمى. وعلى النحو الموضح سابقًا، يُصنع Arthrosamid®/"الجل المائي" في صورة مصفوفة ذات روابط متقاطعة من سلاسل البولي أكريلاميد. المادة النهائية، عند حقنها، لا تحتوي في الأساس على مكونات جسيمية صغيرة، وتم قياس أصغر حجم للجسيمات القابلة للقياس فيها فكان أنها > 300 ميكرومتر، وهو حجم أعلى بكثير من حجم جسيم الميكرون الفردي الذي تم تسجيل أنه متحرّك من الناحية الفسيولوجية.
في الدراسات التي أجريت على الأرانب والخيول، لوحظ وجود خلايا بلعمية وخلايا عملاقة مرتبطة بالجل المائي، ولم يكن هناك دليل على وجود جزيئات جل مائي داخل الجسيمات البلعمية في هذه الخلايا (كريستنسن وآخرون، 2016). وقد أجريت دراسات إضافية لتقييم تصريف العقد الليمفاوية والأنسجة البعيدة عن مواقع حقن الأنسجة الرخوة مع عدم وجود دليل على وجود جل مائي في العقد الليمفاوية المحلية أو في الأعضاء البعيدة (تشارلز ريفر، 2011). جرى وصف إمكانية تنقل الجل المائي من البولي أكريلاميد الذي تصنَعه شركة Contura ومناقشة تلك الإمكانية على نطاق واسع في تقرير التقييم البيولوجي، والذي استُنتِج فيه - استنادًا إلى المطبوعات المنشورة والاختبارات الخاصة بعقار Arthrosamid® - أن الجل المائي من البولي أكريلاميد سيبقى كطعم دائم في الأنسجة تحت الزليلية.
Arthrosamid® - أدلة سريرية وقبل سريرية على iPAAG
جرت متابعة اندماج الجل المائي في الأرانب والخيول لمدة تصل إلى عامين بعد الحقن. فبعد أسبوعين من علاج الخيول، ظهر الجل المائي في صورة طبقة داخلية داخل البطانة الزليليّة مختلطة مع الخلايا الزليليّة المتكاثرة، على غرار الهيستولوجيا التي لوحظَت في نموذج الأرانب. وعند مرور شهر واحد، فلى ما يبدو أن الخلايا الزليليّة انتقلت نحو السطح، وعند مرور 3 أشهر و8 أشهر و24 شهرًا لوحظ نمط مماثل من الاندماج (كريستنسن وآخرون، 2016). وكان الجل المائي موجودًا كمنطقة مندمجة داخل النسيج الخلالي في الأنسجة تحت الزليلية مع شبكة أنسجة حاملة للأوعية الدقيقة وعدد قليل للغاية من الخلايا الالتهابية.
أجريت دراسة هيستوباثولوجية استباقية على أنسجة مأخوذة من المرضى في أثناء الرأب الكلي لمفصل الركبة (TKA). وكان المرضى قد تلقوا العلاج بالجل المائي قبل 5 أشهر-33 شهرًا. ولوحظ وجود نمط هيستولوجي مشابه في جميع الحالات السبع؛ حيث وُجِد أن الجل المائي مُدمج في الغشاء الزليلي، وخلايا البطانة الزليلية الخارجية دخلت الجل وأنشأت طبقة بطانة جديدة. وتم وصف نمط مماثل بعد 9 أشهر من الرأب الكلي لمفصل الركب في إحدى دراسات الحالة (كريستنسن ودوجارد، 2016).
تُسوّق شركة Contura لجلها المائي منذ عام 2001 وأُجري عدد من الدراسات بأوقات متابعة مختلفة لمؤشرات متنوعة. وتتوفر بيانات جُمعَت على مدار فترة طويلة عن جل Contura المائي المصنوع من البولي أكريلاميد في إطار دراسة متابعة مدتها 10 سنوات شملت 104 من المرضى بفيروس نقص المناعة البشرية تم حقنهم بمتوسط 6 مل من الجل المائي Aquamid® لعلاج الضمور الشحمي للوجه. ولم يظهر لدى أي مريض، خلال فترة المتابعة (10 سنوات)، انتقال الجل المائي من موضعه، وكان غالبية المرضى "راضين للغاية" (74.8٪) أو "راضين" (23.4٪) عن النتيجة التجميلية (نيجريدو وآخرون، 2015). كما لوحظ أيضًا أن مظهر الجل المائي مستقر في دراسة متابعة أخرى مدتها ثماني سنوات أُجريت على 25 امرأة تعاني من سلس البول الإجهادي وقد عولجن بالجل المائي Bulkamid®، إذ كان لدى جميع المرضى ترسبات جل مائي من البولي أكريلاميد واضحة في التصوير بالموجات فوق الصوتية المهبلية (موريتسين وآخرون، 2014).
الاستنتاج – استقرار عقار Arthrosamid® ومدى عمره
كما أوضحنا في هذا القسم والأقسام السابقة، أظهرت الدراسات قبل السريرية أن عقار Arthrosamid ®/"الجل المائي" متوافق حيويًا وغير قابل للامتصاص وغير قابل للتحلل الحيوي وغير قابل للانتقال من موضع لآخر (بيلو وآخرون، 2007؛ وتشارلز ريفر، 2011؛ وزاريني وآخرون، 2004). وقد أكدت ذلك البيانات السريرية التي جمعت على مدار مدة طويلة (موريتسين وآخرون، 2014؛ ونيجريدو وآخرون، 2015). ولذلك من المنطقي أن نستنتج أن Arthrosamid® مستقر وآمن طوال عمر الجهاز.
الغرض المقصود من عقار Arthrosamid® كالتالي:
الغرض المقصود من Arthrosamid® |
|
دواعي الاستعمال |
عقار Arthrosamid® مخصص لعلاج أعراض الفُصال العظمي في الركبة لدى البالغين. |
المرض المراد علاجه |
الفُصال العظمي في الركبة. |
المرضى |
المرضى البالغون المصابون بالفُصال العظمي. |
الاستخدام المقصود |
Arthrosamid® مخصص للحقن داخل المفصل في مفصل الركبة. |
المستخدم المستهدف |
Arthrosamid® مُصمَّم للاستخدام على يد طبيب مؤهل على دراية بإجراءات الحقن داخل المفصل، مثل جراحي العظام أو أخصائيي الروماتيزم. |
التأثير على جسم الإنسان |
Arthrosamid® يقلل الألم ويحسن وظيفة الركبة المصابة بالفُصال العظمي. |
الأنسجة الملامسة للجهاز |
مفصل الركبة. |
مدة الاستخدام |
طويل المدى (>30 يومًا)*. |
ملامسة الأغشية المخاطية |
يلامس Arthrosamid® الغشاء الزليلي لمفصل الركبة. |
إجراء جراحي أم غير جراحي |
جراحي. |
قابل للزرع/غير قابل للزرع |
قابل للزرع. |
الاستخدام لمرة واحدة/قابل لإعادة الاستخدام |
الاستخدام لمرة واحدة. |
الجرعة الموصى بها |
6 مل**. |
موانع الاستعمال |
لا ينبغي حقن Arthrosamid® في الحالات التالية:
|
التحذيرات |
|
الاحتياطات المطلوبة من جانب الشركة المصنّعة |
|
الجدول 6: الغرض المقصود من Arthrosamid®. *تُقدَّم بيانات المتابعة السريرية لمدة اثني عشر شهرًا لعقار Arthrosamid® (انظر 5.4.1 و5.4.4)، في حين تتوفر البيانات السريرية التي جمعت على مدار مدة طويلة للجل المائي لشركة Contura لدواعي استعمال أخرى لمدة تصل إلى 8 أو 10 سنوات (3.1.2.10)، وبالتالي من المعقول الاعتقاد بأن هذا الطعم الدائم/الجل المائي مستقر وآمن طوال عمر الجهاز (3.1.2.10).
**تعتمد الجرعة الموصى بها البالغة 6 مل على الحجم الإجمالي للجل المحقون في دراسة "إثبات المفهوم" (2 × 3 مل لغالبية (96٪) المرضى) وعلى البيانات المستقاة من دراسة CON-OA (5.4.4). حقنة واحدة بحجم 6 مل مقارنة بـ2 × 3 مل تقلل من خطر الإصابة بالعدوى، وتُعطى المضادات الحيوية الوقائية مرة واحدة فقط.

هل تريد استخدام عقار Arthrosamid®؟
تسكين الآلام بشكل آمن ومستمر بحقنة واحدة فقط. بادر بالتواصل معنا اليوم لاستخدام Arthrosamid ® (iPAAG) مع مرضى الفُصال العظمي في الركبة.
References
Alhede, M., Er, O., Eickhardt, S., Kragh, K., Alhede, M., Christensen, L.D., Poulsen, S.S., Givskov, M., Christensen, L.H., Hoiby, N., Tvede, M., Bjarnsholt, T., 2014. Bacterial biofilm formation and treatment in soft tissue fillers. Pathogens and disease 70, 339-346.
Altman, D., Ghilotti, F., Bellocco, R., Zetterstrom, J., Kopp Kallner, H., 2017. Transurethral Polyacrylamide Hydrogel Injection Therapy in Women Not Eligible for Midurethral Sling Surgery. Female pelvic medicine & reconstructive surgery 23, 318-323.
Altman, D., Hjern, F., Zetterstrom, J., 2016a. Transanal submucosal polyacrylamide gel injection treatment of anal incontinence: a randomized controlled trial. Acta Obstet Gynecol Scand 95, 528-533.
Altman, R.D., Bedi, A., Karlsson, J., Sancheti, P., Schemitsch, E., 2016b. Product Differences in Intra-articular Hyaluronic Acids for Osteoarthritis of the Knee. The American journal of sports medicine 44, 2158-2165.
Bagga, H., Burkhardt, D., Sambrook, P., March, L., 2006. Longterm effects of intraarticular hyaluronan on synovial fluid in osteoarthritis of the knee. J Rheumatol 33, 946-950.
Balazs, E.A., 2004. Viscosupplementation for treatment of osteoarthritis: from initial discovery to current status and results. Surgical technology international 12, 278-289.
Bellamy, N., Campbell, J., Robinson, V., Gee, T., Bourne, R., Wells, G., 2006. Viscosupplementation for the treatment of osteoarthritis of the knee. The Cochrane database of systematic reviews, Cd005321.
Bellamy, N., Hochberg, M., Tubach, F., Martin-Mola, E., Awada, H., Bombardier, C., Hajjaj-Hassouni, N., Logeart, I., Matucci-Cerinic, M., van de Laar, M., van der Heijde, D., Dougados, M., 2015. Development of multinational definitions of minimal clinically important improvement and patient acceptable symptomatic state in osteoarthritis. Arthritis care & research 67, 972-980.
Bello, G., Jackson, I.T., Keskin, M., Kelly, C., Dajani, K., Studinger, R., Kim, E., Lincoln, D., Silberberg, B., Lee, A., 2007. The Use of Polyacrylamide Gel in Soft Tissue Augmentation: An Experimental Assessment. Plast.Reconstr.Surg 119, 1326-1336.
Belluzzi, E., Stocco, E., Pozzuoli, A., Granzotto, M., Porzionato, A., Vettor, R., De Caro, R., Ruggieri, P., Ramonda, R., Rossato, M., Favero, M., Macchi, V., 2019. Contribution of Infrapatellar Fat Pad and Synovial Membrane to Knee Osteoarthritis Pain. Biomed Res Int 2019, 6390182.
Belmont, P.J., Jr., Goodman, G.P., Waterman, B.R., Bader, J.O., Schoenfeld, A.J., 2014. Thirty-day postoperative complications and mortality following total knee arthroplasty: incidence and risk factors among a national sample of 15,321 patients. The Journal of bone and joint surgery. American volume 96, 20-26.
Benazzo, F., Perticarini, L., Padolino, A., Castelli, A., Gifuni, P., Lovato, M., Manzini, C., Giordan, N., 2016. A multi-centre, open label, long-term follow-up study to evaluate the benefits of a new viscoelastic hydrogel (Hymovis(R)) in the treatment of knee osteoarthritis. European review for medical and pharmacological sciences 20, 959-968.
Bisicchia, S., Bernardi, G., Tudisco, C., 2016. HYADD 4 versus methylprednisolone acetate in symptomatic knee osteoarthritis: a single-centre single blind prospective randomised controlled clinical study with 1-year follow-up. Clinical and experimental rheumatology 34, 857-863.
Bruyere, O., Cooper, C., Pelletier, J.P., Maheu, E., Rannou, F., Branco, J., Luisa Brandi, M., Kanis, J.A., Altman, R.D., Hochberg, M.C., Martel-Pelletier, J., Reginster, J.Y., 2016. A consensus statement on the European Society for Clinical and Economic Aspects of Osteoporosis and Osteoarthritis (ESCEO) algorithm for the management of knee osteoarthritis-From evidence-based medicine to the real-life setting. Seminars in arthritis and rheumatism 45, S3-11.
Bruyere, O., Honvo, G., Veronese, N., Arden, N.K., Branco, J., Curtis, E.M., Al-Daghri, N.M., Herrero-Beaumont, G., Martel-Pelletier, J., Pelletier, J.P., Rannou, F., Rizzoli, R., Roth, R., Uebelhart, D., Cooper, C., Reginster, J.Y., 2019. An updated algorithm recommendation for the management of knee osteoarthritis from the European Society for Clinical and Economic Aspects of Osteoporosis, Osteoarthritis and Musculoskeletal Diseases (ESCEO). Seminars in arthritis and rheumatism 49, 337-350.
Carr, A.J., Robertsson, O., Graves, S., Price, A.J., Arden, N.K., Judge, A., Beard, D.J., 2012. Knee replacement. Lancet 379, 1331-1340.
Charles River 2011. Assessment of local and systemic effects of Bulkamid hydrogel for urethral implantation - a two year follow-up study in sheep. Study No 285465.
Chempilots 2004. Description of the gel's chemical/physical structure, 1-3.
Christensen, L., 2007. Normal and pathologic tissue reactions to soft tissue gel fillers. Dermatol.Surg. 33 Suppl 2, S168-S175.
Christensen, L. 2019. The synovium – interaction with gel endoprosthesis – clinical outcome in OA (unpublished).
Christensen, L., Breiting, V., Bjarnsholt, T., Eickhardt, S., Hogdall, E., Janssen, M., Pallua, N., Zaat, S.A., 2013. Bacterial infection as a likely cause of adverse reactions to polyacrylamide hydrogel fillers in cosmetic surgery. Clinical infectious diseases : an official publication of the Infectious Diseases Society of America 56, 1438-1444.
Christensen, L., Camitz, L., Illigen, K.E., Hansen, M., Sarvaa, R., Conaghan, P.G., 2016. Synovial incorporation of polyacrylamide hydrogel after injection into normal and osteoarthritic animal joints. Osteoarthritis and cartilage / OARS, Osteoarthritis Research Society 24, 1999-2002.
Christensen, L., Daugaard, S., 2016. Histological Appearance of the Synovial Membrane after Treatment of Knee Osteoarthritis with Polyacrylamide Gel Injections: A Case Report. Journal of Arthritis 5, 217.
Christensen, L.H., 2009. Host tissue interaction, fate, and risks of degradable and nondegradable gel fillers. Dermatol.Surg. 35 Suppl 2, 1612-1619.
Christensen, L.H., Nielsen, J.B., Mouritsen, L., Sorensen, M., Lose, G., 2008. Tissue integration of polyacrylamide hydrogel: an experimental study of periurethral, perivesical, and mammary gland tissue in the pig. Dermatol.Surg. 34 Suppl 1, S68-S77.
de Clifford, L.T., Lowe, J.N., McKellar, C.D., Bolwell, C., David, F., 2019. Use of a 2.5% Cross-Linked Polyacrylamide Hydrogel in the Management of Joint Lameness in a Population of Flat Racing Thoroughbreds: A Pilot Study. Journal of Equine Veterinary Science 77, 57-62.
De Santis, G., Pignatti, M., Baccarani, A., Pedone, A., Spaggiari, A., Orlando, G., Guaraldi, G., 2012. Long-term efficacy and safety of polyacrylamide hydrogel injection in the treatment of human immunodeficiency virus-related facial lipoatrophy: a 5-year follow-up. Plast Reconstr Surg 129, 101-109.
Di Matteo, B., Vandenbulcke, F., Vitale, N.D., Iacono, F., Ashmore, K., Marcacci, M., Kon, E., 2019. Minimally Manipulated Mesenchymal Stem Cells for the Treatment of Knee Osteoarthritis: A Systematic Review of Clinical Evidence. Stem cells international 2019, 1735242.
Divine, J.G., Zazulak, B.T., Hewett, T.E., 2006. Viscosupplementation for knee osteoarthritis: a systematic review. Clinical orthopaedics and related research 455, 113-122.
Fam, H., Bryant, J.T., Kontopoulou, M., 2007. Rheological properties of synovial fluids. Biorheology 44, 59-74.
Faundez, E., Vega, N., Vera, E., Vega, P., Sepulveda, D., Wortsman, X., 2017. Clinical and color Doppler ultrasound evaluation of polyacrylamide injection in HIV patients with severe facial lipoatrophy secondary to antiretroviral therapy. Skin research and technology : official journal of International Society for Bioengineering and the Skin (ISBS) [and] International Society for Digital Imaging of Skin (ISDIS) [and] International Society for Skin Imaging (ISSI) 23, 243-248.
Felson, D.T., Lawrence, R.C., Dieppe, P.A., Hirsch, R., Helmick, C.G., Jordan, J.M., Kington, R.S., Lane, N.E., Nevitt, M.C., Zhang, Y., Sowers, M., McAlindon, T., Spector, T.D., Poole, A.R., Yanovski, S.Z., Ateshian, G., Sharma, L., Buckwalter, J.A., Brandt, K.D., Fries, J.F., 2000. Osteoarthritis: new insights. Part 1: the disease and its risk factors. Annals of internal medicine 133, 635-646.
Goldman, D.T., Piechowiak, R., Nissman, D., Bagla, S., Isaacson, A., 2018. Current Concepts and Future Directions of Minimally Invasive Treatment for Knee Pain. Current rheumatology reports 20, 54.
Gomis, A., Pawlak, M., Balazs, E.A., Schmidt, R.F., Belmonte, C., 2004. Effects of different molecular weight elastoviscous hyaluronan solutions on articular nociceptive afferents. Arthritis and rheumatism 50, 314-326.
Hansen, M.F., Lose, G., Kesmodel, U.S., Gradel, K.O., 2017. A national population-based cohort study of urethral injection therapy for female stress and mixed urinary incontinence: the Danish Urogynaecological Database, 2007-2011. Int Urogynecol J, doi: 10.1007/s00192-00017-03265-z.
Hartkopp, A. 2015. Injection of non-degradable polyacrylamide gel into the knee joint has long-term effect on osteoarthritis symptoms – a pilot study (A2 Clinic of Rheumatology and Sports Medicine A/S, Hillerød, Denmark).
He, W.W., Kuang, M.J., Zhao, J., Sun, L., Lu, B., Wang, Y., Ma, J.X., Ma, X.L., 2017. Efficacy and safety of intraarticular hyaluronic acid and corticosteroid for knee osteoarthritis: A meta-analysis. International journal of surgery (London, England) 39, 95-103.
Henriksen, M., Overgaard, A., Hartkopp, A., Bliddal, H., 2018. Intra-articular 2.5% polyacrylamide hydrogel for the treatment of knee osteoarthritis: an observational proof-of-concept cohort study. Clinical and experimental rheumatology 36, 1082-1085.
Hermans, J., Bierma-Zeinstra, S.M.A., Bos, P.K., Niesten, D.D., Verhaar, J.A.N., Reijman, M., 2019. The effectiveness of high molecular weight hyaluronic acid for knee osteoarthritis in patients in the working age: a randomised controlled trial. BMC musculoskeletal disorders 20, 196.
Hochberg, M.C., Altman, R.D., April, K.T., Benkhalti, M., Guyatt, G., McGowan, J., Towheed, T., Welch, V., Wells, G., Tugwell, P., 2012. American College of Rheumatology 2012 recommendations for the use of nonpharmacologic and pharmacologic therapies in osteoarthritis of the hand, hip, and knee. Arthritis care & research 64, 465-474.
Hollenz, M., Stolte, M., Leodolter, A., Labenz, J., 2006. NSAID-associated dyspepsia and ulcers: a prospective cohort study in primary care. Digestive diseases (Basel, Switzerland) 24, 189-194.
Hootman, J.M., Helmick, C.G., 2006. Projections of US prevalence of arthritis and associated activity limitations. Arthritis and rheumatism 54, 226-229.
Itkonen Freitas, A.M., Mentula, M., Rahkola-Soisalo, P., Tulokas, S., Mikkola, T.S., 2020. Tension-Free Vaginal Tape Surgery versus Polyacrylamide Hydrogel Injection for Primary Stress Urinary Incontinence: A Randomized Clinical Trial. J Urol 203, 372-378.
Jette, D.U., Hunter, S.J., Burkett, L., Langham, B., Logerstedt, D.S., Piuzzi, N.S., Poirier, N.M., Radach, L.J.L., Ritter, J.E., Scalzitti, D.A., Stevens-Lapsley, J.E., Tompkins, J., Zeni, J., Jr., 2020. Physical Therapist Management of Total Knee Arthroplasty. Phys Ther 100, 1603-1631.
Jevsevar, D., Donnelly, P., Brown, G.A., Cummins, D.S., 2015. Viscosupplementation for Osteoarthritis of the Knee: A Systematic Review of the Evidence. The Journal of bone and joint surgery. American volume 97, 2047-2060.
Jevsevar, D.S., Brown, G.A., Jones, D.L., Matzkin, E.G., Manner, P.A., Mooar, P., Schousboe, J.T., Stovitz, S., Sanders, J.O., Bozic, K.J., Goldberg, M.J., Martin, W.R., 3rd, Cummins, D.S., Donnelly, P., Woznica, A., Gross, L., 2013. The American Academy of Orthopaedic Surgeons evidence-based guideline on: treatment of osteoarthritis of the knee, 2nd edition. https://www.aaos.org/research/guidelines/treatmentofosteoarthritisofthekneeguideline.pdf. The Journal of bone and joint surgery. American volume 95, 1885-1886.
Kasi, A.D., Pergialiotis, V., Perrea, D.N., Khunda, A., Doumouchtsis, S.K., 2016. Polyacrylamide hydrogel (Bulkamid(R)) for stress urinary incontinence in women: a systematic review of the literature. Int Urogynecol J 27, 367-375.
Kohn, M.D., Sassoon, A.A., Fernando, N.D., 2016. Classifications in Brief: Kellgren-Lawrence Classification of Osteoarthritis. Clinical orthopaedics and related research 474, 1886-1893.
Kolasinski, S.L., Neogi, T., Hochberg, M.C., Oatis, C., Guyatt, G., Block, J., Callahan, L., Copenhaver, C., Dodge, C., Felson, D., Gellar, K., Harvey, W.F., Hawker, G., Herzig, E., Kwoh, C.K., Nelson, A.E., Samuels, J., Scanzello, C., White, D., Wise, B., Altman, R.D., DiRenzo, D., Fontanarosa, J., Giradi, G., Ishimori, M., Misra, D., Shah, A.A., Shmagel, A.K., Thoma, L.M., Turgunbaev, M., Turner, A.S., Reston, J., 2020. 2019 American College of Rheumatology/Arthritis Foundation Guideline for the Management of Osteoarthritis of the Hand, Hip, and Knee. Arthritis care & research 72, 149-162.
Krhut, J., Martan, A., Jurakova, M., Nemec, D., Masata, J., Zvara, P., 2016. Treatment of stress urinary incontinence using polyacrylamide hydrogel in women after radiotherapy: 1-year follow-up. Int Urogynecol J 27, 301-305.
Langworthy, M.J., Saad, A., Langworthy, N.M., 2010. Conservative treatment modalities and outcomes for osteoarthritis: the concomitant pyramid of treatment. The Physician and sportsmedicine 38, 133-145.
Leighton, R., Akermark, C., Therrien, R., Richardson, J.B., Andersson, M., Todman, M.G., Arden, N.K., 2014. NASHA hyaluronic acid vs. methylprednisolone for knee osteoarthritis: a prospective, multi-centre, randomized, non-inferiority trial. Osteoarthritis and cartilage / OARS, Osteoarthritis Research Society 22, 17-25.
Leighton, R., Fitzpatrick, J., Smith, H., Crandall, D., Flannery, C.R., Conrozier, T., 2018. Systematic clinical evidence review of NASHA (Durolane hyaluronic acid) for the treatment of knee osteoarthritis. Open Access Rheumatol 10, 43-54.
Leone Roberti Maggiore, U., Alessandri, F., Medica, M., Gabelli, M., Venturini, P.L., Ferrero, S., 2013. Outpatient periurethral injections of polyacrylamide hydrogel for the treatment of female stress urinary incontinence: effectiveness and safety. Archives of gynecology and obstetrics 288, 131-137.
Liddle, A.D., Judge, A., Pandit, H., Murray, D.W., 2014. Adverse outcomes after total and unicompartmental knee replacement in 101,330 matched patients: a study of data from the National Joint Registry for England and Wales. Lancet 384, 1437-1445.
Lowe, J.N., de Clifford, L., McKellar, K., 2016. Intra-articular 2.5% Polyacrylamide Hydrogel (PAAG) for the Treatment of Osteoarthritis in 54 Thoroughbred Racehorses: A Prospective Study. Poster presented at the 38th Bain Fallon Memorial Lectures, Melbourne, Australia run by the Equine Veterinarians Australia, the special interest branch of the Australian Veterinary Association.
Maheu, E., Bannuru, R.R., Herrero-Beaumont, G., Allali, F., Bard, H., Migliore, A., 2019. Why we should definitely include intra-articular hyaluronic acid as a therapeutic option in the management of knee osteoarthritis: Results of an extensive critical literature review. Seminars in arthritis and rheumatism 48, 563-572.
Maheu, E., Rannou, F., Reginster, J.Y., 2016. Efficacy and safety of hyaluronic acid in the management of osteoarthritis: Evidence from real-life setting trials and surveys. Seminars in arthritis and rheumatism 45, S28-33.
Marsland, D., Mumith, A., Barlow, I.W., 2014. Systematic review: the safety of intra-articular corticosteroid injection prior to total knee arthroplasty. The Knee 21, 6-11.
Martan, A., Masata, J., Svabik, K., Krhut, J., 2014. Transurethral injection of polyacrylamide hydrogel (Bulkamid((R))) for the treatment of female stress or mixed urinary incontinence. European journal of obstetrics, gynecology, and reproductive biology 178, 199-202.
Mathiessen, A., Conaghan, P.G., 2017. Synovitis in osteoarthritis: current understanding with therapeutic implications. Arthritis research & therapy 19, 18.
McAlindon, T.E., Bannuru, R.R., Sullivan, M.C., Arden, N.K., Berenbaum, F., Bierma-Zeinstra, S.M., Hawker, G.A., Henrotin, Y., Hunter, D.J., Kawaguchi, H., Kwoh, K., Lohmander, S., Rannou, F., Roos, E.M., Underwood, M., 2014. OARSI guidelines for the non-surgical management of knee osteoarthritis. Osteoarthritis and cartilage / OARS, Osteoarthritis Research Society 22, 363-388.
McGrory, B.J., Weber, K.L., Jevsevar, D.S., Sevarino, K., 2016. Surgical Management of Osteoarthritis of the Knee: Evidence-based Guideline. The Journal of the American Academy of Orthopaedic Surgeons 24, e87-93.
Miller, L.E., Block, J.E., 2013. US-Approved Intra-Articular Hyaluronic Acid Injections are Safe and Effective in Patients with Knee Osteoarthritis: Systematic Review and Meta-Analysis of Randomized, Saline-Controlled Trials. Clinical medicine insights. Arthritis and musculoskeletal disorders 6, 57-63.
Mohr, S., Marthaler, C., Imboden, S., Monga, A., Mueller, M.D., Kuhn, A., 2017. Bulkamid (PAHG) in mixed urinary incontinence: What is the outcome? Int Urogynecol J 28, 1657-1661.
Mohr, S., Siegenthaler, M., Mueller, M.D., Kuhn, A., 2013. Bulking agents: an analysis of 500 cases and review of the literature. Int Urogynecol J 24, 241-247.
Mouritsen, L., Lose, G., Moller-Bek, K., 2014. Long-term follow-up after urethral injection with polyacrylamide hydrogel for female stress incontinence. Acta Obstet Gynecol Scand 93, 209-212.
National Clinical Guideline Centre. 2014. National Institute for Health and Clinical Excellence: Guidance. https://www.ncbi.nlm.nih.gov/books/NBK248069/pdf/Bookshelf_NBK248069.pdf, In: Osteoarthritis: Care and Management in Adults. National Institute for Health and Care Excellence (UK), National Clinical Guideline Centre, 2014., London.
Negredo, E., Puig, J., Ornelas, A., Echeverria, P., Bonjoch, A., Estany, C., Higueras, C., Gonzalez-Mestre, V., Clotet, B., 2015. Ten-Year Safety with Polyacrylamide Gel Used to Correct Facial Lipoatrophy in HIV-Infected Patients. AIDS Res Hum Retroviruses 31, 817-821.
Overgaard, A., Bliddal, H., Henriksen, M., 2019. Safety of Intra-Articular Polyacrylamide Hydrogel for the Treatment of Knee Osteoarthritis Symptoms: A Retrospective Case Series. Clin Ortho Adv Res J: COARJ-100001.
Pai, A., Al-Singary, W., 2015. Durability, safety and efficacy of polyacrylamide hydrogel (Bulkamid®) in the management of stress and mixed urinary incontinence: three year follow up outcomes. Cent European J Urol 68, 428-433.
Pallua, N., Wolter, T.P., 2010. A 5-year assessment of safety and aesthetic results after facial soft-tissue augmentation with polyacrylamide hydrogel (Aquamid): a prospective multicenter study of 251 patients. Plast.Reconstr.Surg. 125, 1797-1804.
Petterson, S.C., Plancher, K.D., 2019. Single intra-articular injection of lightly cross-linked hyaluronic acid reduces knee pain in symptomatic knee osteoarthritis: a multicenter, double-blind, randomized, placebo-controlled trial. Knee surgery, sports traumatology, arthroscopy : official journal of the ESSKA 27, 1992-2002.
Phillips, M., Vannabouathong, C., Devji, T., Patel, R., Gomes, Z., Patel, A., Dixon, M., Bhandari, M., 2020. Differentiating factors of intra-articular injectables have a meaningful impact on knee osteoarthritis outcomes: a network meta-analysis. Knee surgery, sports traumatology, arthroscopy : official journal of the ESSKA 28, 3031-3039.
Price, A.J., Alvand, A., Troelsen, A., Katz, J.N., Hooper, G., Gray, A., Carr, A., Beard, D., 2018. Knee replacement. Lancet 392, 1672-1682.
Rauso, R., 2015. 5-year study of a polyacrylamide hydrogel-based filler for rehabilitation of HIV-related facial lipoatrophy. Aesthet Surg J 35, 1021-1029.
Rauso, R., Califano, L., Rugge, L., Chirico, F., Tartaro, G., 2018. Late Onset Complications Secondary to Polyacrylamide Hydrogel-Based Filler for Rehabilitation of HIV-Related Facial Lipoatropy. Aesthet Surg J 38, Np170-np174.
Rutjes, A.W., Juni, P., da Costa, B.R., Trelle, S., Nuesch, E., Reichenbach, S., 2012. Viscosupplementation for osteoarthritis of the knee: a systematic review and meta-analysis. Annals of internal medicine
157, 180-191.
Rydell, N., Butler, J., Balazs, E.A., 1970. Hyaluronic acid in synovial fluid. VI. Effect of intra-articular injection of hyaluronic acid on the clinical symptoms of arthritis in track horses. Acta veterinaria Scandinavica 11, 139-155.
Shen, D., Chen, M., Chen, K., Wang, T., Lu, L., Yang, X., 2018. Efficacy of hyaluronic acid after knee arthroscopy: A systematic review and meta-analysis. Journal of rehabilitation medicine 50, 860-865.
Siddiqui, Z.A., Abboudi, H., Crawford, R., Shah, S., 2017. Intraurethral bulking agents for the management of female stress urinary incontinence: a systematic review. Int Urogynecol J.
Skou, S.T., Roos, E.M., Laursen, M.B., Rathleff, M.S., Arendt-Nielsen, L., Rasmussen, S., Simonsen, O., 2018. Total knee replacement and non-surgical treatment of knee osteoarthritis: 2-year outcome from two parallel randomized controlled trials. Osteoarthritis and cartilage / OARS, Osteoarthritis Research Society 26, 1170-1180.
Skou, S.T., Roos, E.M., Laursen, M.B., Rathleff, M.S., Arendt-Nielsen, L., Simonsen, O., Rasmussen, S., 2015. A Randomized, Controlled Trial of Total Knee Replacement. The New England journal of medicine 373, 1597-1606.
Sokol, E.R., Karram, M.M., Dmochowski, R., 2014. Efficacy and safety of polyacrylamide hydrogel for the treatment of female stress incontinence: a randomized, prospective, multicenter North American study. J Urol 192, 843-849.
Steinhaus, M.E., Christ, A.B., Cross, M.B., 2017. Total Knee Arthroplasty for Knee Osteoarthritis: Support for a Foregone Conclusion? HSS journal : the musculoskeletal journal of Hospital for Special Surgery 13, 207-210.
Sun, S.F., Hsu, C.W., Lin, H.S., Liou, I.H., Chen, Y.H., Hung, C.L., 2017. Comparison of Single Intra-Articular Injection of Novel Hyaluronan (HYA-JOINT Plus) with Synvisc-One for Knee Osteoarthritis: A Randomized, Controlled, Double-Blind Trial of Efficacy and Safety. The Journal of bone and joint surgery. American volume 99, 462-471.
Tammachote, N., Kanitnate, S., Yakumpor, T., Panichkul, P., 2016. Intra-Articular, Single-Shot Hylan G-F 20 Hyaluronic Acid Injection Compared with Corticosteroid in Knee Osteoarthritis: A Double-Blind, Randomized Controlled Trial. The Journal of bone and joint surgery. American volume 98, 885-892.
Tnibar, A., Britt Persson, A., Elvang Jensen, H., 2017. Mechanisms of Action of an Intraarticular 2.5% Polyacrylamide Hydrogel (Arthramid Vet) in a Goat Model of Osteoarthritis: Preliminary Observations. SM Journal of Biomedical Engineering 3, 1022.
Tnibar, A., Persson, A.B., Nielsen, H., Svalastoga, E., Westrup, U., McEvoy, F., Knudsen, J., Thomsen, P.D., Berg, L.C., Jacobsen, S., Christensen, L.H., 2014a. Evaluation of a polyacrylamide hydrogel in the treatment of induced osteoarthritis in a goat model: a randomized controlled pilot study. Abs. 871. Osteoarthritis and Cartilage 22, S477.
Tnibar, A., Schougaard, H., Camitz, L., Rasmussen, J., Koene, M., Jahn, W., Markussen, B., 2015. An international multi-centre prospective study on the efficacy of an intraarticular polyacrylamide hydrogel in horses with osteoarthritis: a 24 months follow-up. Acta veterinaria Scandinavica 57, 20.
Tnibar, A., Schougaard, H., Koene, M., Christensen, L., Markussen, B., 2014b. A controlled clinical trial on the efficacy of an intra-articular Polyacrylamide Hydrogel in horses with osteoarthritis [abstract]. Veterinary Surgery 43, E138.
Tonbul, M., Adas, M., Bekmezci, T., Kara, A.D., 2014. Intra-articular polyacrylamide hydrogel injections are not innocent. Case reports in orthopedics 2014, 150709.
Toozs-Hobson, P., Al-Singary, W., Fynes, M., Tegerstedt, G., Lose, G., 2012. Two-year follow-up of an open-label multicenter study of polyacrylamide hydrogel (Bulkamid(R)) for female stress and stress-predominant mixed incontinence. Int. Urogynecol. J.
Trojian, T.H., Concoff, A.L., Joy, S.M., Hatzenbuehler, J.R., Saulsberry, W.J., Coleman, C.I., 2016. AMSSM scientific statement concerning viscosupplementation injections for knee osteoarthritis: importance for individual patient outcomes. British journal of sports medicine 50, 84-92.
Vallejo, A., Garcia-Ruano, A.A., Pinilla, C., Castellano, M., Deleyto, E., Perez-Cano, R., 2017. "Comparing efficacy and costs of four facial fillers in HIV-associated lipodystrophy: a clinical trial.". Plast Reconstr Surg.
Vecchioli-Scaldazza, C., 2014. Polyacrylamide hydrogel (Bulkamid®) in female patients of 80 or more years with urinary incontinence. Int Braz J Urol. 40, 37-43.
Wilson, M.G., Kelley, K., Thornhill, T.S., 1990. Infection as a complication of total knee-replacement arthroplasty. Risk factors and treatment in sixty-seven cases. The Journal of bone and joint surgery. American volume 72, 878-883.
Yan, C.H., Chan, W.L., Yuen, W.H., Yung, P.S., Ip, K.Y., Fan, J.C., Chiu, K.Y., 2015. Efficacy and safety of hylan G-F 20 injection in treatment of knee osteoarthritis in Chinese patients: results of a prospective, multicentre, longitudinal study. Hong Kong medical journal = Xianggang yi xue za zhi 21, 327-332.
Zar, V.V., Zagorodniy, N.V., Martinov, D.V., 2012. Effectiveness and safety of injectable endprosthetics of sinovial fluid by cross-linked polimer Noltrex for treatment OA knee. European Journal of Musculoskeletal Diseases 1, 23-32.
Zarini, E., Supino, R., Pratesi, G., Laccabue, D., Tortoreto, M., Scanziani, E., Ghisleni, G., Paltrinieri, S., Tunesi, G., Nava, M., 2004. Biocompatibility and tissue interactions of a new filler material for medical use. Plast.Reconstr.Surg. 114, 934-942.
Zhao, H., Liu, H., Liang, X., Li, Y., Wang, J., Liu, C., 2016. Hylan G-F 20 Versus Low Molecular Weight Hyaluronic Acids for Knee Osteoarthritis: A Meta-Analysis. BioDrugs : clinical immunotherapeutics, biopharmaceuticals and gene therapy 30, 387-396.
Zivanovic, I., Rautenberg, O., Lobodasch, K., von Bunau, G., Walser, C., Viereck, V., 2017. Urethral bulking for recurrent stress urinary incontinence after midurethral sling failure. Neurourol Urodyn 36, 722-726.