La ciencia de Arthrosamid® (iPAAG)
Un tratamiento novedoso para adultos con osteoartritis de rodilla
Arthrosamid® es un gel hidrofílico, no absorbible, no biodegradable, inyectable y transparente formado por un pilar de poliacrilamida firmemente vinculado y no biodegradable (2,5 %) y agua no pirogénica (97,5 %).
Arthrosamid® se suministra como una jeringa de 1 ml pre-llenada, de uso único y estéril, sellada con un cierre luer lock y una funda. Está destinado a ser inyectado intraarticularmente en la articulación de la rodilla con una aguja estéril de 21G x 2 pulgadas (0,8 x 50 mm).
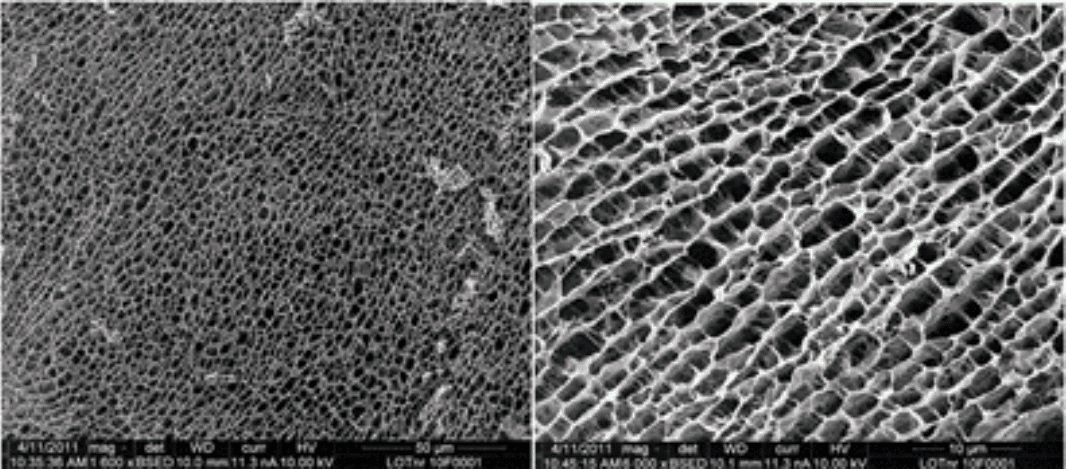
La Figura 1 muestra la estructura tridimensional del hidrogel de poliacrilamida. La estructura ligera y uniforme en forma de panal de miel proporciona una matriz para el crecimiento celular.
Descripción química de la poliacrilamida
Como se ha descrito anteriormente, el hidrogel Arthrosamid® consta del 2,5 % de poliacrilamida reticulada seca y un 97,5 % de agua no pirogénica. Durante la síntesis, la N,N'-metilenbisacrilamida se polimeriza con acrilamida, creando interconexiones entre las cadenas de poliacrilamida.
El hidrogel de poliacrilamida reticulada se sintetiza en un proceso de polimerización donde las unidades repetidas de acrilamida se vinculan en una reacción en cadena.
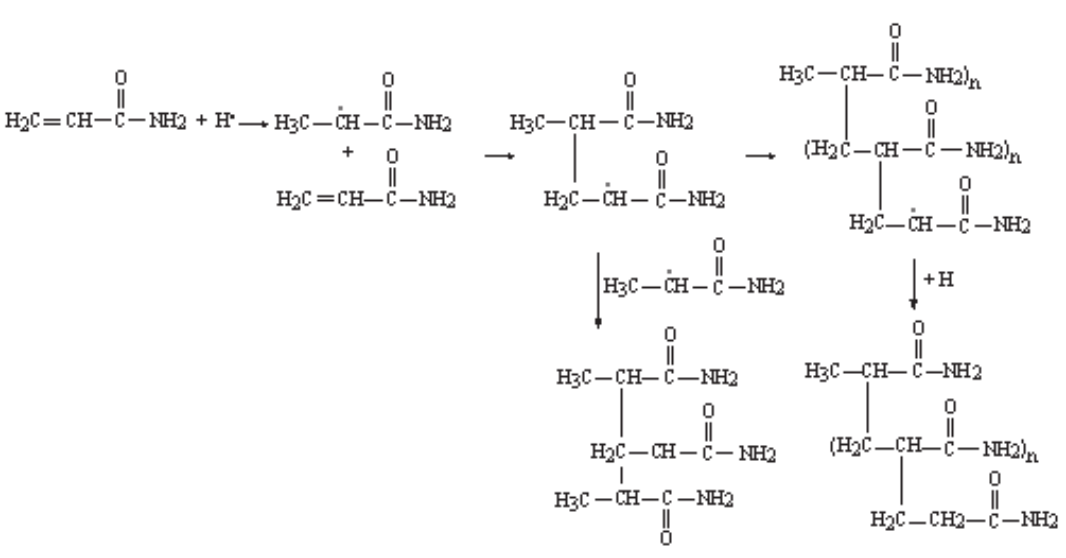
La reacción en cadena implica un principio de iniciador redox, donde un iniciador de persulfato de amonio (AMPS) genera un radical libre que añade un monómero de acrilamida obteniendo un electrón a partir del doble enlace de la acrilamida, formando así un único enlace carbono-carbono con la acrilamida. Esto deja un electrón sin compartir para la posterior adición de monómeros de acrilamida como se ilustra en la Figura 2 de la derecha.
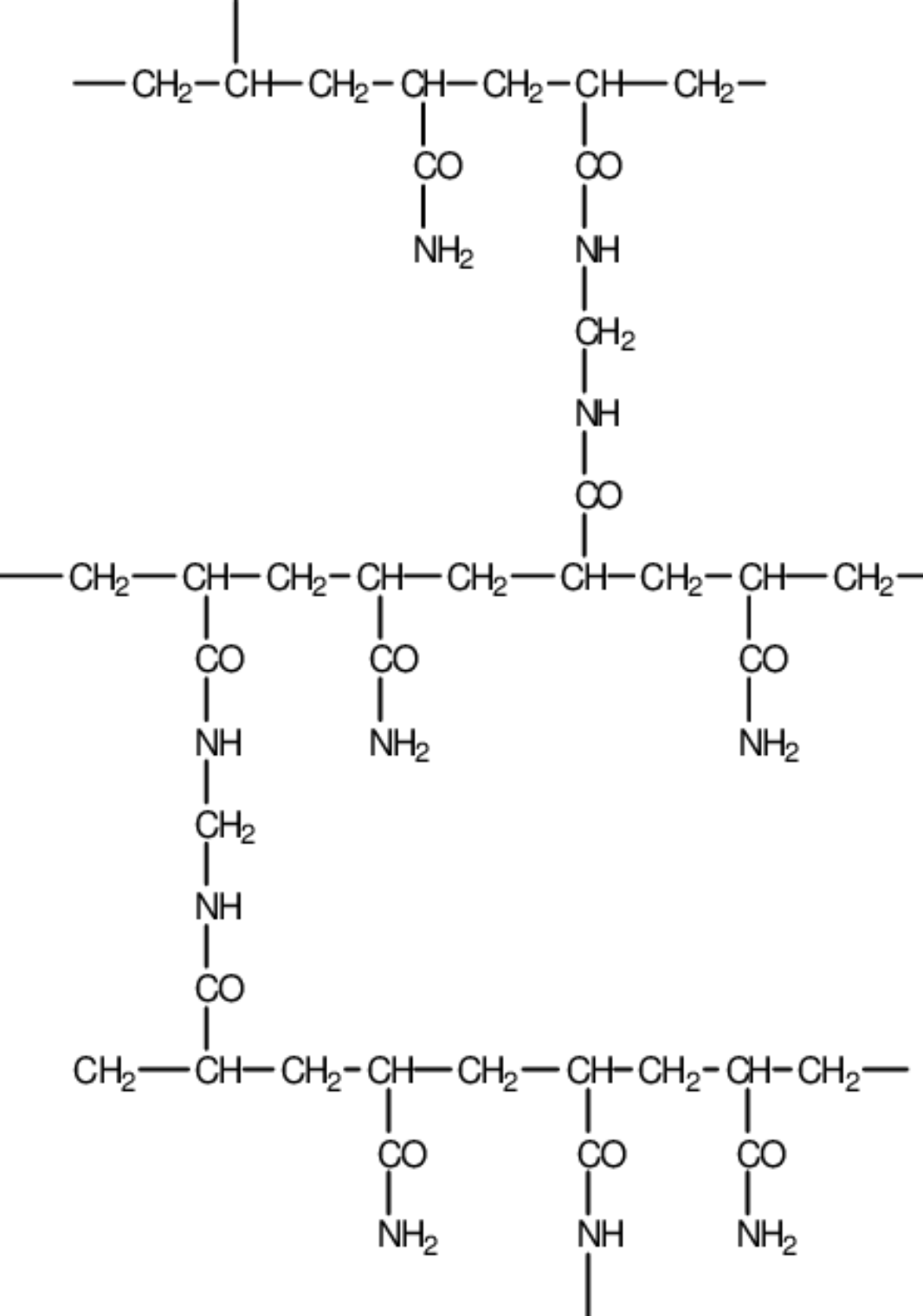
Se producirá la ramificación del eje linear carbono-carbono de poliacrilamida debido a la presencia de un agente reticulante, el monómero N,N'-metilenbisacrilamida (MBAM), como se ilustra en la Figura 3.
Tras la ramificación de las cadenas centrales de poliacrilamida, se forma una red tridimensional de poliacrilamida reticulada, en vez de cadenas lineales no conectadas de poliacrilamida.
Materiales de Arthrosamid® y biocompatibilidad
Arthrosamid® no incorpora una sustancia medicamentosa, tejidos o productos sanguíneos.
Los materiales usados en Arthrosamid® se listan a continuación (Tabla 2).
Parte del dispositivo |
Material |
Contacto con el cuerpo |
|
|---|---|---|---|
Gel |
Gel hidrofílico que consiste en aproximadamente el 2,5 % de poliacrilamida reticulada y el 97,5 % de agua no pirogénica |
Articulación de la rodilla |
|
Jeringa |
Cilindro |
Polipropileno |
Piel* |
Émbolo |
Policarbonato |
Piel* |
|
Tope de caucho |
Caucho de silicona |
Piel* |
|
Lubricante |
Aceite de silicona |
Piel* |
|
Funda de la punta |
Polipropileno |
Piel* |
|
Tabla 2. Materiales del dispositivo. *La jeringa será manipulada por el usuario, que llevará guantes protectores. Normalmente ni el paciente ni el usuario deberían entrar en contacto con la jeringa. El tope de caucho y el lubricante no están expuestos y por tanto el riesgo de entrar en contacto con ellos es incluso inferior que para las partes expuestas de la jeringa.
Se han realizado pruebas de biocompatibilidad de acuerdo con ISO 10993-1 para los productos de hidrogel existentes de Contura, y las pruebas que se consideran relevantes para Arthrosamid® se resumen a continuación (Tabla 3) y se describen en detalle en el Informe de Evaluación Biológica (BER) - Arthrosamid®.
Resultado de la evaluación biológica |
Referencia estándar |
Prueba y número de prueba |
Fecha del informe |
Resultado |
|---|---|---|---|---|
Citotoxicidad |
ISO 10993-5:2009 USP 29 |
Hidrogel B: Prueba de citotoxicidad in vitro Nº 16/368-030C |
2017 |
Superada |
Sensibilización |
ISO 10993-10: 2010 |
Evaluación de hipersensibilidad por contacto en cobaya (prueba de maximización), Ensayo local de ganglio linfático en ratones Nº 517557 |
2017 |
Superada |
Hidrogel B: Ensayo local de ganglio linfático (sensibilización de la piel) Nº 77691) |
2017 |
|||
Irritación o reactividad intracutánea |
ISO 10993-10: 2010 |
Prueba de reactividad intracutánea en conejos Nº 77693 |
2017 |
Superada |
Toxicidad sistémica (aguda) |
ISO 10993-11: 2017 / 10993-12: 2012 USP 151 |
Prueba de pirogenicidad mediada de material Nº APS-GZJ009-ST01 |
2018 |
Superada |
Toxicidad subcrónica (toxicidad subaguda) |
ISO 10993-6:2007 |
Los resultados de toxicidad sistémica para toxicidad subcrónica fueron examinados en el estudio de implantación de dos años en ovejas Nº 285465 |
2017 |
Superada |
Genotoxicidad |
ISO 10993-3: 2014 |
Ensayo de mutación inversa bacteriana (test de Ames) Nº 16/368-007M |
2017 |
Superada |
Prueba de aberración cromosómica in vitro en mamíferos Nº 16/368-020C |
2017 |
|||
Prueba In vivo de micronúcleos en eritrocitos en mamíferos Nº 16/368-013E |
2017 APR07 |
|||
Implantación |
ISO 10993-6:2007 |
Estudio de implantación de dos años en ovejas Nº 285465 |
2017 |
Superada |
Tabla 3. Estudios de biocompatibilidad (y estudio de implantación) realizado sobre el hidrogel de Contura
En base a las pruebas realizadas, Arthrosamid® se considera biocompatible y adecuado para el contacto a largo plazo con el cuerpo.
Estabilidad y durabilidad de Arthrosamid®
La estabilidad de los hidrogeles de poliacrilamida de Contura se describe y aborda ampliamente en el Informe de Evaluación Biológica (BER) - Arthrosamid®, y a continuación se proporciona un resumen de las pruebas estabilidad que investigan la hidrólisis potencial, y el estrés oxidativo y físico sobre el «Hidrogel B» (Tabla 5). Como se revisa en el BER, la degradación enzimática de la poliacrilamida ha sido probada en varios sistemas de fermentación enzimática, pero no se observó degradación.
| Condición | Prueba | Resultado | Referencia de prueba |
|---|---|---|---|
| Hidrólisis y estrés oxidativo | Se incubaron muestras duplicadas de Hidrogel B 24 horas a 37ºC en disolventes hipotónicos e isotónicos no oxidativos, moderadamente oxidativos y extremadamente oxidativos. Se compararon disolventes neutrales con pH 2 ajustado y no ajustado. Las muestras fueron analizadas por HPLC. | El Hidrogel B no mostró ninguna tendencia de formar acrilamida monomérica bajo condiciones de prueba no oxidativa y oxidativa y ácido hidrolítico agresivo. | ChemPilot 2018 |
| Estrés físico | Una configuración experimental expuso el hidrogel a una tensión de cizallamiento mecánico extrema en un procedimiento de mezcla con cuchillo. | La tensión mecánica extrema no provocó degradación del hidrogel en monómeros de acrilamida. La tensión mecánica extrema, como la mezcla con cuchillo, no se experimentó durante condiciones fisiológicas. | Contura (011.INR.00025) |
Tabla 5. Estudios de estabilidad realizados sobre el hidrogel de Contura («Hidrogel B»).
Se ha visto que el hidrogel de poliacrilamida es estable y no se degrada bajo las condiciones de prueba.
Estabilidad de Arthrosamid® - Migración
El potencial de migración del hidrogel de poliacrilamida se ha estudiado ampliamente, según revisión del BER y en el informe «Evaluación del potencial de migración y degradación de Arthrosamid® tras su administración intraarticular». En pocas palabras, en relación con la inyección intraarticular, se ha observado que pequeñas partículas (8 µm o menos) están sometidas a fagocitosis, y fluirán con el líquido sinovial a través de las intersecciones de espacios en el epitelio sinovial y eventualmente se distribuirán sistémicamente, mientras que las partículas más grandes (> 8-17 µm) se encapsulan con el tiempo y permanecen inmóviles dentro de los tejidos blandos indefinidamente. Como se ha descrito previamente, Arthrosamid®/«Hidrogel» está formado como una matriz reticulada de cadenas de poliacrilamida. El material final, cuando se inyecta, no tiene esencialmente componentes de partículas pequeñas, y el tamaño medible más pequeño de la partícula fue medido a > 300 μm, que está bien por encima del tamaño de partícula de una sola micra que ha sido reportado como fisiológicamente móvil.
En estudios con conejos y caballos, se observaron macrófagos y células gigantes asociadas con el hidrogel, y no había evidencias de partículas de hidrogel en fagosomas en estas células (Christensen et al., 2016). Se han realizado estudios adicionales para evaluar los ganglios linfáticos de drenaje y el tejido distante del tejido blando de los puntos de inyección sin evidencias de hidrogel en los ganglios linfático de drenaje locales o en órganos distantes (Charles River, 2011). La migración potencial de los hidrogeles de poliacrilamida de Contura se describe y aborda ampliamente en el BER, donde, según la literatura publicada y las pruebas específicas de Arthrosamid®, se concluye que el hidrogel de poliacrilamida permanecerá como un implante permanente en los tenidos subsinoviales.
Arthrosamid® - Evidencias clínicas y pre clínicas del iPAAG
En conejos y caballos, se ha realizado un seguimiento de la integración del hidrogel durante un máximo de dos años después de la inyección. En caballos, dos semanas tras el tratamiento, el hidrogel aparecía como una capa interna dentro del revestimiento sinovial entremezclado con células sinoviales proliferantes, similar a la histología vista en el modelo de conejos. Al mes, las células sinoviales aparentemente se reubicaron hacia la superficie, y a 3, 8 y 24 meses, se observó un patrón similar de integración (Christensen et al., 2016). El hidrogel estaba presente como una zona integrada dentro del intersticio subsinovial con una red de tejido con vasos y muy pocas células inflamatorias.
Se ha realizado un estudio histopatológico prospectivo sobre tejido extirpado de pacientes durante una artroplastia total de rodilla (TKA). Los pacientes habían recibido tratamiento con el hidrogel entre 5 y 33 meses antes. Se observó un patrón histológico similar en los siete casos. Se encontró que el hidrogel se integró en la membrana sinovial y las células externas del revestimiento sinovial entraron en el gel y establecieron una capa de revestimiento de novo. Se describió un patrón similar nueve meses tras una TKA en un estudio de caso (Christensen y Daugaard, 2016).
Los hidrogeles de Contura se han comercializado desde el año 2001, y se han realizado numerosos estudios clínicos para varias indicaciones con diferentes tiempos de seguimiento. Los datos a largo plazo sobre el hidrogel de poliacrilamida de Contura están disponibles de un estudio de seguimiento de 10 años que incluye 104 pacientes de VIH inyectados con una media de 6 ml del hidrogel Aquamid® para el tratamiento de la lipoatrofia facial. En el seguimiento (10 años), ningún paciente presentó migración del hidrogel y la mayoría de los pacientes estuvieron «altamente satisfechos) (74,8 %) o «satisfechos» (23,4 %) con el resultado cosmético (Negredo et al., 2015). La apariencia estable del hidrogel también se observó en un estudio de seguimiento de ocho años de 25 mujeres con incontinencia urinaria por estrés, que fueron tratadas con el hidrogel Bulkamid®, donde todas las pacientes tenían depósitos de hidrogel de poliacrilamida visibles en una ultrasonografía vaginal (Mouritsen et al., 2014).
Conclusión - Estabilidad y durabilidad de Arthrosamid®
Como se ha descrito en esta y en las secciones previas, los estudios pre-clínicos han demostrado que Arthrosamid®/«Hidrogel» es biocompatible, no absorbible, no biodegradable, y no migratorio (Bello et al., 2007; Charles River, 2011; Zarini et al., 2004). Los datos clínicos a largo plazo han confirmado esto (Mouritsen et al., 2014; Negredo et al., 2015). Es por tanto razonable concluir que Arthrosamid® es estable y seguro durante la vida útil del dispositivo.
El fin previsto de Arthrosamid® se resume a continuación:
Fin previsto de Arthrosamid® |
|
Indicación |
Arthrosamid® se ha diseñado para su uso en el tratamiento sintomático de la osteoartritis de rodilla en adultos. |
Patología a tratar |
Osteoartritis de rodilla. |
Población de pacientes |
Pacientes adultos diagnosticados con osteoartritis. |
Aplicación prevista |
Arthrosamid® debe inyectarse intraarticularmente en la articulación de la rodilla. |
Usuario previsto |
Arthrosamid® debe ser usado por un médico cualificado familiarizado con los procedimientos de inyección intraarticular, como cirujanos ortopédicos o reumatólogos. |
Efecto sobre el cuerpo humano |
Arthrosamid® reduce el dolor y mejora la función de la rodilla afectada por la osteoartritis. |
Tejidos e contacto con el dispositivo |
Articulación de la rodilla. |
Duración del uso |
A largo plazo (>30 días)*. |
Contacto con membranas mucosas |
Arthrosamid® está en contacto con la membrana sinovial de la articulación de la rodilla. |
Invasivo/no invasivo |
Invasivo. |
Implantable/no implantable |
Implantable. |
Uso único/reutilizable |
Uso único. |
Dosis recomendada |
6 ml**. |
Contraindicaciones |
Arthrosamid® no debe inyectarse:
|
Advertencias |
|
Precauciones requeridas por el fabricante |
|
Tabla 6. Fin previsto de Arthrosamid® *Se presentan datos de seguimiento clínico de 12 meses para Arthrosamid® (véase 5.4.1 y 5.4.4), aunque existen datos clínicos a largo plazo de hidrogeles de Contura para otras indicaciones de hasta ocho o 10 años (3.1.2.10), y es por tanto razonable creer que este implante/hidrogel permanente es estable y seguro durante la vida útil del dispositivo (3.1.2.10).
**La dosis recomendada de 6 ml se basa en el volumen total de gel inyectado en el estudio de «prueba de concepto» (2 x 3 ml para la mayoría (96 %) de los pacientes) y en los datos del estudio CON-OA (5.4.4). Una inyección de 6 ml en comparación con 2 x 3 ml reduce el riesgo de infección, y los antibióticos profilácticos solo se administran una vez.

¿Quiere usar Arthrosamid®?
Alivio seguro y sostenido del dolor en una única inyección. Póngase en contacto con nosotros para usar el iPAAG Arthrosamid® en sus pacientes con osteoartritis de rodilla hoy mismo.
References
Alhede, M., Er, O., Eickhardt, S., Kragh, K., Alhede, M., Christensen, L.D., Poulsen, S.S., Givskov, M., Christensen, L.H., Hoiby, N., Tvede, M., Bjarnsholt, T., 2014. Bacterial biofilm formation and treatment in soft tissue fillers. Pathogens and disease 70, 339-346.
Altman, D., Ghilotti, F., Bellocco, R., Zetterstrom, J., Kopp Kallner, H., 2017. Transurethral Polyacrylamide Hydrogel Injection Therapy in Women Not Eligible for Midurethral Sling Surgery. Female pelvic medicine & reconstructive surgery 23, 318-323.
Altman, D., Hjern, F., Zetterstrom, J., 2016a. Transanal submucosal polyacrylamide gel injection treatment of anal incontinence: a randomized controlled trial. Acta Obstet Gynecol Scand 95, 528-533.
Altman, R.D., Bedi, A., Karlsson, J., Sancheti, P., Schemitsch, E., 2016b. Product Differences in Intra-articular Hyaluronic Acids for Osteoarthritis of the Knee. The American journal of sports medicine 44, 2158-2165.
Bagga, H., Burkhardt, D., Sambrook, P., March, L., 2006. Longterm effects of intraarticular hyaluronan on synovial fluid in osteoarthritis of the knee. J Rheumatol 33, 946-950.
Balazs, E.A., 2004. Viscosupplementation for treatment of osteoarthritis: from initial discovery to current status and results. Surgical technology international 12, 278-289.
Bellamy, N., Campbell, J., Robinson, V., Gee, T., Bourne, R., Wells, G., 2006. Viscosupplementation for the treatment of osteoarthritis of the knee. The Cochrane database of systematic reviews, Cd005321.
Bellamy, N., Hochberg, M., Tubach, F., Martin-Mola, E., Awada, H., Bombardier, C., Hajjaj-Hassouni, N., Logeart, I., Matucci-Cerinic, M., van de Laar, M., van der Heijde, D., Dougados, M., 2015. Development of multinational definitions of minimal clinically important improvement and patient acceptable symptomatic state in osteoarthritis. Arthritis care & research 67, 972-980.
Bello, G., Jackson, I.T., Keskin, M., Kelly, C., Dajani, K., Studinger, R., Kim, E., Lincoln, D., Silberberg, B., Lee, A., 2007. The Use of Polyacrylamide Gel in Soft Tissue Augmentation: An Experimental Assessment. Plast.Reconstr.Surg 119, 1326-1336.
Belluzzi, E., Stocco, E., Pozzuoli, A., Granzotto, M., Porzionato, A., Vettor, R., De Caro, R., Ruggieri, P., Ramonda, R., Rossato, M., Favero, M., Macchi, V., 2019. Contribution of Infrapatellar Fat Pad and Synovial Membrane to Knee Osteoarthritis Pain. Biomed Res Int 2019, 6390182.
Belmont, P.J., Jr., Goodman, G.P., Waterman, B.R., Bader, J.O., Schoenfeld, A.J., 2014. Thirty-day postoperative complications and mortality following total knee arthroplasty: incidence and risk factors among a national sample of 15,321 patients. The Journal of bone and joint surgery. American volume 96, 20-26.
Benazzo, F., Perticarini, L., Padolino, A., Castelli, A., Gifuni, P., Lovato, M., Manzini, C., Giordan, N., 2016. A multi-centre, open label, long-term follow-up study to evaluate the benefits of a new viscoelastic hydrogel (Hymovis(R)) in the treatment of knee osteoarthritis. European review for medical and pharmacological sciences 20, 959-968.
Bisicchia, S., Bernardi, G., Tudisco, C., 2016. HYADD 4 versus methylprednisolone acetate in symptomatic knee osteoarthritis: a single-centre single blind prospective randomised controlled clinical study with 1-year follow-up. Clinical and experimental rheumatology 34, 857-863.
Bruyere, O., Cooper, C., Pelletier, J.P., Maheu, E., Rannou, F., Branco, J., Luisa Brandi, M., Kanis, J.A., Altman, R.D., Hochberg, M.C., Martel-Pelletier, J., Reginster, J.Y., 2016. A consensus statement on the European Society for Clinical and Economic Aspects of Osteoporosis and Osteoarthritis (ESCEO) algorithm for the management of knee osteoarthritis-From evidence-based medicine to the real-life setting. Seminars in arthritis and rheumatism 45, S3-11.
Bruyere, O., Honvo, G., Veronese, N., Arden, N.K., Branco, J., Curtis, E.M., Al-Daghri, N.M., Herrero-Beaumont, G., Martel-Pelletier, J., Pelletier, J.P., Rannou, F., Rizzoli, R., Roth, R., Uebelhart, D., Cooper, C., Reginster, J.Y., 2019. An updated algorithm recommendation for the management of knee osteoarthritis from the European Society for Clinical and Economic Aspects of Osteoporosis, Osteoarthritis and Musculoskeletal Diseases (ESCEO). Seminars in arthritis and rheumatism 49, 337-350.
Carr, A.J., Robertsson, O., Graves, S., Price, A.J., Arden, N.K., Judge, A., Beard, D.J., 2012. Knee replacement. Lancet 379, 1331-1340.
Charles River 2011. Assessment of local and systemic effects of Bulkamid hydrogel for urethral implantation - a two year follow-up study in sheep. Study No 285465.
Chempilots 2004. Description of the gel's chemical/physical structure, 1-3.
Christensen, L., 2007. Normal and pathologic tissue reactions to soft tissue gel fillers. Dermatol.Surg. 33 Suppl 2, S168-S175.
Christensen, L. 2019. The synovium – interaction with gel endoprosthesis – clinical outcome in OA (unpublished).
Christensen, L., Breiting, V., Bjarnsholt, T., Eickhardt, S., Hogdall, E., Janssen, M., Pallua, N., Zaat, S.A., 2013. Bacterial infection as a likely cause of adverse reactions to polyacrylamide hydrogel fillers in cosmetic surgery. Clinical infectious diseases : an official publication of the Infectious Diseases Society of America 56, 1438-1444.
Christensen, L., Camitz, L., Illigen, K.E., Hansen, M., Sarvaa, R., Conaghan, P.G., 2016. Synovial incorporation of polyacrylamide hydrogel after injection into normal and osteoarthritic animal joints. Osteoarthritis and cartilage / OARS, Osteoarthritis Research Society 24, 1999-2002.
Christensen, L., Daugaard, S., 2016. Histological Appearance of the Synovial Membrane after Treatment of Knee Osteoarthritis with Polyacrylamide Gel Injections: A Case Report. Journal of Arthritis 5, 217.
Christensen, L.H., 2009. Host tissue interaction, fate, and risks of degradable and nondegradable gel fillers. Dermatol.Surg. 35 Suppl 2, 1612-1619.
Christensen, L.H., Nielsen, J.B., Mouritsen, L., Sorensen, M., Lose, G., 2008. Tissue integration of polyacrylamide hydrogel: an experimental study of periurethral, perivesical, and mammary gland tissue in the pig. Dermatol.Surg. 34 Suppl 1, S68-S77.
de Clifford, L.T., Lowe, J.N., McKellar, C.D., Bolwell, C., David, F., 2019. Use of a 2.5% Cross-Linked Polyacrylamide Hydrogel in the Management of Joint Lameness in a Population of Flat Racing Thoroughbreds: A Pilot Study. Journal of Equine Veterinary Science 77, 57-62.
De Santis, G., Pignatti, M., Baccarani, A., Pedone, A., Spaggiari, A., Orlando, G., Guaraldi, G., 2012. Long-term efficacy and safety of polyacrylamide hydrogel injection in the treatment of human immunodeficiency virus-related facial lipoatrophy: a 5-year follow-up. Plast Reconstr Surg 129, 101-109.
Di Matteo, B., Vandenbulcke, F., Vitale, N.D., Iacono, F., Ashmore, K., Marcacci, M., Kon, E., 2019. Minimally Manipulated Mesenchymal Stem Cells for the Treatment of Knee Osteoarthritis: A Systematic Review of Clinical Evidence. Stem cells international 2019, 1735242.
Divine, J.G., Zazulak, B.T., Hewett, T.E., 2006. Viscosupplementation for knee osteoarthritis: a systematic review. Clinical orthopaedics and related research 455, 113-122.
Fam, H., Bryant, J.T., Kontopoulou, M., 2007. Rheological properties of synovial fluids. Biorheology 44, 59-74.
Faundez, E., Vega, N., Vera, E., Vega, P., Sepulveda, D., Wortsman, X., 2017. Clinical and color Doppler ultrasound evaluation of polyacrylamide injection in HIV patients with severe facial lipoatrophy secondary to antiretroviral therapy. Skin research and technology : official journal of International Society for Bioengineering and the Skin (ISBS) [and] International Society for Digital Imaging of Skin (ISDIS) [and] International Society for Skin Imaging (ISSI) 23, 243-248.
Felson, D.T., Lawrence, R.C., Dieppe, P.A., Hirsch, R., Helmick, C.G., Jordan, J.M., Kington, R.S., Lane, N.E., Nevitt, M.C., Zhang, Y., Sowers, M., McAlindon, T., Spector, T.D., Poole, A.R., Yanovski, S.Z., Ateshian, G., Sharma, L., Buckwalter, J.A., Brandt, K.D., Fries, J.F., 2000. Osteoarthritis: new insights. Part 1: the disease and its risk factors. Annals of internal medicine 133, 635-646.
Goldman, D.T., Piechowiak, R., Nissman, D., Bagla, S., Isaacson, A., 2018. Current Concepts and Future Directions of Minimally Invasive Treatment for Knee Pain. Current rheumatology reports 20, 54.
Gomis, A., Pawlak, M., Balazs, E.A., Schmidt, R.F., Belmonte, C., 2004. Effects of different molecular weight elastoviscous hyaluronan solutions on articular nociceptive afferents. Arthritis and rheumatism 50, 314-326.
Hansen, M.F., Lose, G., Kesmodel, U.S., Gradel, K.O., 2017. A national population-based cohort study of urethral injection therapy for female stress and mixed urinary incontinence: the Danish Urogynaecological Database, 2007-2011. Int Urogynecol J, doi: 10.1007/s00192-00017-03265-z.
Hartkopp, A. 2015. Injection of non-degradable polyacrylamide gel into the knee joint has long-term effect on osteoarthritis symptoms – a pilot study (A2 Clinic of Rheumatology and Sports Medicine A/S, Hillerød, Denmark).
He, W.W., Kuang, M.J., Zhao, J., Sun, L., Lu, B., Wang, Y., Ma, J.X., Ma, X.L., 2017. Efficacy and safety of intraarticular hyaluronic acid and corticosteroid for knee osteoarthritis: A meta-analysis. International journal of surgery (London, England) 39, 95-103.
Henriksen, M., Overgaard, A., Hartkopp, A., Bliddal, H., 2018. Intra-articular 2.5% polyacrylamide hydrogel for the treatment of knee osteoarthritis: an observational proof-of-concept cohort study. Clinical and experimental rheumatology 36, 1082-1085.
Hermans, J., Bierma-Zeinstra, S.M.A., Bos, P.K., Niesten, D.D., Verhaar, J.A.N., Reijman, M., 2019. The effectiveness of high molecular weight hyaluronic acid for knee osteoarthritis in patients in the working age: a randomised controlled trial. BMC musculoskeletal disorders 20, 196.
Hochberg, M.C., Altman, R.D., April, K.T., Benkhalti, M., Guyatt, G., McGowan, J., Towheed, T., Welch, V., Wells, G., Tugwell, P., 2012. American College of Rheumatology 2012 recommendations for the use of nonpharmacologic and pharmacologic therapies in osteoarthritis of the hand, hip, and knee. Arthritis care & research 64, 465-474.
Hollenz, M., Stolte, M., Leodolter, A., Labenz, J., 2006. NSAID-associated dyspepsia and ulcers: a prospective cohort study in primary care. Digestive diseases (Basel, Switzerland) 24, 189-194.
Hootman, J.M., Helmick, C.G., 2006. Projections of US prevalence of arthritis and associated activity limitations. Arthritis and rheumatism 54, 226-229.
Itkonen Freitas, A.M., Mentula, M., Rahkola-Soisalo, P., Tulokas, S., Mikkola, T.S., 2020. Tension-Free Vaginal Tape Surgery versus Polyacrylamide Hydrogel Injection for Primary Stress Urinary Incontinence: A Randomized Clinical Trial. J Urol 203, 372-378.
Jette, D.U., Hunter, S.J., Burkett, L., Langham, B., Logerstedt, D.S., Piuzzi, N.S., Poirier, N.M., Radach, L.J.L., Ritter, J.E., Scalzitti, D.A., Stevens-Lapsley, J.E., Tompkins, J., Zeni, J., Jr., 2020. Physical Therapist Management of Total Knee Arthroplasty. Phys Ther 100, 1603-1631.
Jevsevar, D., Donnelly, P., Brown, G.A., Cummins, D.S., 2015. Viscosupplementation for Osteoarthritis of the Knee: A Systematic Review of the Evidence. The Journal of bone and joint surgery. American volume 97, 2047-2060.
Jevsevar, D.S., Brown, G.A., Jones, D.L., Matzkin, E.G., Manner, P.A., Mooar, P., Schousboe, J.T., Stovitz, S., Sanders, J.O., Bozic, K.J., Goldberg, M.J., Martin, W.R., 3rd, Cummins, D.S., Donnelly, P., Woznica, A., Gross, L., 2013. The American Academy of Orthopaedic Surgeons evidence-based guideline on: treatment of osteoarthritis of the knee, 2nd edition. https://www.aaos.org/research/guidelines/treatmentofosteoarthritisofthekneeguideline.pdf. The Journal of bone and joint surgery. American volume 95, 1885-1886.
Kasi, A.D., Pergialiotis, V., Perrea, D.N., Khunda, A., Doumouchtsis, S.K., 2016. Polyacrylamide hydrogel (Bulkamid(R)) for stress urinary incontinence in women: a systematic review of the literature. Int Urogynecol J 27, 367-375.
Kohn, M.D., Sassoon, A.A., Fernando, N.D., 2016. Classifications in Brief: Kellgren-Lawrence Classification of Osteoarthritis. Clinical orthopaedics and related research 474, 1886-1893.
Kolasinski, S.L., Neogi, T., Hochberg, M.C., Oatis, C., Guyatt, G., Block, J., Callahan, L., Copenhaver, C., Dodge, C., Felson, D., Gellar, K., Harvey, W.F., Hawker, G., Herzig, E., Kwoh, C.K., Nelson, A.E., Samuels, J., Scanzello, C., White, D., Wise, B., Altman, R.D., DiRenzo, D., Fontanarosa, J., Giradi, G., Ishimori, M., Misra, D., Shah, A.A., Shmagel, A.K., Thoma, L.M., Turgunbaev, M., Turner, A.S., Reston, J., 2020. 2019 American College of Rheumatology/Arthritis Foundation Guideline for the Management of Osteoarthritis of the Hand, Hip, and Knee. Arthritis care & research 72, 149-162.
Krhut, J., Martan, A., Jurakova, M., Nemec, D., Masata, J., Zvara, P., 2016. Treatment of stress urinary incontinence using polyacrylamide hydrogel in women after radiotherapy: 1-year follow-up. Int Urogynecol J 27, 301-305.
Langworthy, M.J., Saad, A., Langworthy, N.M., 2010. Conservative treatment modalities and outcomes for osteoarthritis: the concomitant pyramid of treatment. The Physician and sportsmedicine 38, 133-145.
Leighton, R., Akermark, C., Therrien, R., Richardson, J.B., Andersson, M., Todman, M.G., Arden, N.K., 2014. NASHA hyaluronic acid vs. methylprednisolone for knee osteoarthritis: a prospective, multi-centre, randomized, non-inferiority trial. Osteoarthritis and cartilage / OARS, Osteoarthritis Research Society 22, 17-25.
Leighton, R., Fitzpatrick, J., Smith, H., Crandall, D., Flannery, C.R., Conrozier, T., 2018. Systematic clinical evidence review of NASHA (Durolane hyaluronic acid) for the treatment of knee osteoarthritis. Open Access Rheumatol 10, 43-54.
Leone Roberti Maggiore, U., Alessandri, F., Medica, M., Gabelli, M., Venturini, P.L., Ferrero, S., 2013. Outpatient periurethral injections of polyacrylamide hydrogel for the treatment of female stress urinary incontinence: effectiveness and safety. Archives of gynecology and obstetrics 288, 131-137.
Liddle, A.D., Judge, A., Pandit, H., Murray, D.W., 2014. Adverse outcomes after total and unicompartmental knee replacement in 101,330 matched patients: a study of data from the National Joint Registry for England and Wales. Lancet 384, 1437-1445.
Lowe, J.N., de Clifford, L., McKellar, K., 2016. Intra-articular 2.5% Polyacrylamide Hydrogel (PAAG) for the Treatment of Osteoarthritis in 54 Thoroughbred Racehorses: A Prospective Study. Poster presented at the 38th Bain Fallon Memorial Lectures, Melbourne, Australia run by the Equine Veterinarians Australia, the special interest branch of the Australian Veterinary Association.
Maheu, E., Bannuru, R.R., Herrero-Beaumont, G., Allali, F., Bard, H., Migliore, A., 2019. Why we should definitely include intra-articular hyaluronic acid as a therapeutic option in the management of knee osteoarthritis: Results of an extensive critical literature review. Seminars in arthritis and rheumatism 48, 563-572.
Maheu, E., Rannou, F., Reginster, J.Y., 2016. Efficacy and safety of hyaluronic acid in the management of osteoarthritis: Evidence from real-life setting trials and surveys. Seminars in arthritis and rheumatism 45, S28-33.
Marsland, D., Mumith, A., Barlow, I.W., 2014. Systematic review: the safety of intra-articular corticosteroid injection prior to total knee arthroplasty. The Knee 21, 6-11.
Martan, A., Masata, J., Svabik, K., Krhut, J., 2014. Transurethral injection of polyacrylamide hydrogel (Bulkamid((R))) for the treatment of female stress or mixed urinary incontinence. European journal of obstetrics, gynecology, and reproductive biology 178, 199-202.
Mathiessen, A., Conaghan, P.G., 2017. Synovitis in osteoarthritis: current understanding with therapeutic implications. Arthritis research & therapy 19, 18.
McAlindon, T.E., Bannuru, R.R., Sullivan, M.C., Arden, N.K., Berenbaum, F., Bierma-Zeinstra, S.M., Hawker, G.A., Henrotin, Y., Hunter, D.J., Kawaguchi, H., Kwoh, K., Lohmander, S., Rannou, F., Roos, E.M., Underwood, M., 2014. OARSI guidelines for the non-surgical management of knee osteoarthritis. Osteoarthritis and cartilage / OARS, Osteoarthritis Research Society 22, 363-388.
McGrory, B.J., Weber, K.L., Jevsevar, D.S., Sevarino, K., 2016. Surgical Management of Osteoarthritis of the Knee: Evidence-based Guideline. The Journal of the American Academy of Orthopaedic Surgeons 24, e87-93.
Miller, L.E., Block, J.E., 2013. US-Approved Intra-Articular Hyaluronic Acid Injections are Safe and Effective in Patients with Knee Osteoarthritis: Systematic Review and Meta-Analysis of Randomized, Saline-Controlled Trials. Clinical medicine insights. Arthritis and musculoskeletal disorders 6, 57-63.
Mohr, S., Marthaler, C., Imboden, S., Monga, A., Mueller, M.D., Kuhn, A., 2017. Bulkamid (PAHG) in mixed urinary incontinence: What is the outcome? Int Urogynecol J 28, 1657-1661.
Mohr, S., Siegenthaler, M., Mueller, M.D., Kuhn, A., 2013. Bulking agents: an analysis of 500 cases and review of the literature. Int Urogynecol J 24, 241-247.
Mouritsen, L., Lose, G., Moller-Bek, K., 2014. Long-term follow-up after urethral injection with polyacrylamide hydrogel for female stress incontinence. Acta Obstet Gynecol Scand 93, 209-212.
National Clinical Guideline Centre. 2014. National Institute for Health and Clinical Excellence: Guidance. https://www.ncbi.nlm.nih.gov/books/NBK248069/pdf/Bookshelf_NBK248069.pdf, In: Osteoarthritis: Care and Management in Adults. National Institute for Health and Care Excellence (UK), National Clinical Guideline Centre, 2014., London.
Negredo, E., Puig, J., Ornelas, A., Echeverria, P., Bonjoch, A., Estany, C., Higueras, C., Gonzalez-Mestre, V., Clotet, B., 2015. Ten-Year Safety with Polyacrylamide Gel Used to Correct Facial Lipoatrophy in HIV-Infected Patients. AIDS Res Hum Retroviruses 31, 817-821.
Overgaard, A., Bliddal, H., Henriksen, M., 2019. Safety of Intra-Articular Polyacrylamide Hydrogel for the Treatment of Knee Osteoarthritis Symptoms: A Retrospective Case Series. Clin Ortho Adv Res J: COARJ-100001.
Pai, A., Al-Singary, W., 2015. Durability, safety and efficacy of polyacrylamide hydrogel (Bulkamid®) in the management of stress and mixed urinary incontinence: three year follow up outcomes. Cent European J Urol 68, 428-433.
Pallua, N., Wolter, T.P., 2010. A 5-year assessment of safety and aesthetic results after facial soft-tissue augmentation with polyacrylamide hydrogel (Aquamid): a prospective multicenter study of 251 patients. Plast.Reconstr.Surg. 125, 1797-1804.
Petterson, S.C., Plancher, K.D., 2019. Single intra-articular injection of lightly cross-linked hyaluronic acid reduces knee pain in symptomatic knee osteoarthritis: a multicenter, double-blind, randomized, placebo-controlled trial. Knee surgery, sports traumatology, arthroscopy : official journal of the ESSKA 27, 1992-2002.
Phillips, M., Vannabouathong, C., Devji, T., Patel, R., Gomes, Z., Patel, A., Dixon, M., Bhandari, M., 2020. Differentiating factors of intra-articular injectables have a meaningful impact on knee osteoarthritis outcomes: a network meta-analysis. Knee surgery, sports traumatology, arthroscopy : official journal of the ESSKA 28, 3031-3039.
Price, A.J., Alvand, A., Troelsen, A., Katz, J.N., Hooper, G., Gray, A., Carr, A., Beard, D., 2018. Knee replacement. Lancet 392, 1672-1682.
Rauso, R., 2015. 5-year study of a polyacrylamide hydrogel-based filler for rehabilitation of HIV-related facial lipoatrophy. Aesthet Surg J 35, 1021-1029.
Rauso, R., Califano, L., Rugge, L., Chirico, F., Tartaro, G., 2018. Late Onset Complications Secondary to Polyacrylamide Hydrogel-Based Filler for Rehabilitation of HIV-Related Facial Lipoatropy. Aesthet Surg J 38, Np170-np174.
Rutjes, A.W., Juni, P., da Costa, B.R., Trelle, S., Nuesch, E., Reichenbach, S., 2012. Viscosupplementation for osteoarthritis of the knee: a systematic review and meta-analysis. Annals of internal medicine
157, 180-191.
Rydell, N., Butler, J., Balazs, E.A., 1970. Hyaluronic acid in synovial fluid. VI. Effect of intra-articular injection of hyaluronic acid on the clinical symptoms of arthritis in track horses. Acta veterinaria Scandinavica 11, 139-155.
Shen, D., Chen, M., Chen, K., Wang, T., Lu, L., Yang, X., 2018. Efficacy of hyaluronic acid after knee arthroscopy: A systematic review and meta-analysis. Journal of rehabilitation medicine 50, 860-865.
Siddiqui, Z.A., Abboudi, H., Crawford, R., Shah, S., 2017. Intraurethral bulking agents for the management of female stress urinary incontinence: a systematic review. Int Urogynecol J.
Skou, S.T., Roos, E.M., Laursen, M.B., Rathleff, M.S., Arendt-Nielsen, L., Rasmussen, S., Simonsen, O., 2018. Total knee replacement and non-surgical treatment of knee osteoarthritis: 2-year outcome from two parallel randomized controlled trials. Osteoarthritis and cartilage / OARS, Osteoarthritis Research Society 26, 1170-1180.
Skou, S.T., Roos, E.M., Laursen, M.B., Rathleff, M.S., Arendt-Nielsen, L., Simonsen, O., Rasmussen, S., 2015. A Randomized, Controlled Trial of Total Knee Replacement. The New England journal of medicine 373, 1597-1606.
Sokol, E.R., Karram, M.M., Dmochowski, R., 2014. Efficacy and safety of polyacrylamide hydrogel for the treatment of female stress incontinence: a randomized, prospective, multicenter North American study. J Urol 192, 843-849.
Steinhaus, M.E., Christ, A.B., Cross, M.B., 2017. Total Knee Arthroplasty for Knee Osteoarthritis: Support for a Foregone Conclusion? HSS journal : the musculoskeletal journal of Hospital for Special Surgery 13, 207-210.
Sun, S.F., Hsu, C.W., Lin, H.S., Liou, I.H., Chen, Y.H., Hung, C.L., 2017. Comparison of Single Intra-Articular Injection of Novel Hyaluronan (HYA-JOINT Plus) with Synvisc-One for Knee Osteoarthritis: A Randomized, Controlled, Double-Blind Trial of Efficacy and Safety. The Journal of bone and joint surgery. American volume 99, 462-471.
Tammachote, N., Kanitnate, S., Yakumpor, T., Panichkul, P., 2016. Intra-Articular, Single-Shot Hylan G-F 20 Hyaluronic Acid Injection Compared with Corticosteroid in Knee Osteoarthritis: A Double-Blind, Randomized Controlled Trial. The Journal of bone and joint surgery. American volume 98, 885-892.
Tnibar, A., Britt Persson, A., Elvang Jensen, H., 2017. Mechanisms of Action of an Intraarticular 2.5% Polyacrylamide Hydrogel (Arthramid Vet) in a Goat Model of Osteoarthritis: Preliminary Observations. SM Journal of Biomedical Engineering 3, 1022.
Tnibar, A., Persson, A.B., Nielsen, H., Svalastoga, E., Westrup, U., McEvoy, F., Knudsen, J., Thomsen, P.D., Berg, L.C., Jacobsen, S., Christensen, L.H., 2014a. Evaluation of a polyacrylamide hydrogel in the treatment of induced osteoarthritis in a goat model: a randomized controlled pilot study. Abs. 871. Osteoarthritis and Cartilage 22, S477.
Tnibar, A., Schougaard, H., Camitz, L., Rasmussen, J., Koene, M., Jahn, W., Markussen, B., 2015. An international multi-centre prospective study on the efficacy of an intraarticular polyacrylamide hydrogel in horses with osteoarthritis: a 24 months follow-up. Acta veterinaria Scandinavica 57, 20.
Tnibar, A., Schougaard, H., Koene, M., Christensen, L., Markussen, B., 2014b. A controlled clinical trial on the efficacy of an intra-articular Polyacrylamide Hydrogel in horses with osteoarthritis [abstract]. Veterinary Surgery 43, E138.
Tonbul, M., Adas, M., Bekmezci, T., Kara, A.D., 2014. Intra-articular polyacrylamide hydrogel injections are not innocent. Case reports in orthopedics 2014, 150709.
Toozs-Hobson, P., Al-Singary, W., Fynes, M., Tegerstedt, G., Lose, G., 2012. Two-year follow-up of an open-label multicenter study of polyacrylamide hydrogel (Bulkamid(R)) for female stress and stress-predominant mixed incontinence. Int. Urogynecol. J.
Trojian, T.H., Concoff, A.L., Joy, S.M., Hatzenbuehler, J.R., Saulsberry, W.J., Coleman, C.I., 2016. AMSSM scientific statement concerning viscosupplementation injections for knee osteoarthritis: importance for individual patient outcomes. British journal of sports medicine 50, 84-92.
Vallejo, A., Garcia-Ruano, A.A., Pinilla, C., Castellano, M., Deleyto, E., Perez-Cano, R., 2017. "Comparing efficacy and costs of four facial fillers in HIV-associated lipodystrophy: a clinical trial.". Plast Reconstr Surg.
Vecchioli-Scaldazza, C., 2014. Polyacrylamide hydrogel (Bulkamid®) in female patients of 80 or more years with urinary incontinence. Int Braz J Urol. 40, 37-43.
Wilson, M.G., Kelley, K., Thornhill, T.S., 1990. Infection as a complication of total knee-replacement arthroplasty. Risk factors and treatment in sixty-seven cases. The Journal of bone and joint surgery. American volume 72, 878-883.
Yan, C.H., Chan, W.L., Yuen, W.H., Yung, P.S., Ip, K.Y., Fan, J.C., Chiu, K.Y., 2015. Efficacy and safety of hylan G-F 20 injection in treatment of knee osteoarthritis in Chinese patients: results of a prospective, multicentre, longitudinal study. Hong Kong medical journal = Xianggang yi xue za zhi 21, 327-332.
Zar, V.V., Zagorodniy, N.V., Martinov, D.V., 2012. Effectiveness and safety of injectable endprosthetics of sinovial fluid by cross-linked polimer Noltrex for treatment OA knee. European Journal of Musculoskeletal Diseases 1, 23-32.
Zarini, E., Supino, R., Pratesi, G., Laccabue, D., Tortoreto, M., Scanziani, E., Ghisleni, G., Paltrinieri, S., Tunesi, G., Nava, M., 2004. Biocompatibility and tissue interactions of a new filler material for medical use. Plast.Reconstr.Surg. 114, 934-942.
Zhao, H., Liu, H., Liang, X., Li, Y., Wang, J., Liu, C., 2016. Hylan G-F 20 Versus Low Molecular Weight Hyaluronic Acids for Knee Osteoarthritis: A Meta-Analysis. BioDrugs : clinical immunotherapeutics, biopharmaceuticals and gene therapy 30, 387-396.
Zivanovic, I., Rautenberg, O., Lobodasch, K., von Bunau, G., Walser, C., Viereck, V., 2017. Urethral bulking for recurrent stress urinary incontinence after midurethral sling failure. Neurourol Urodyn 36, 722-726.