Die Wissenschaft von Arthrosamid® (iPAAG)
Eine neue Behandlung für Erwachsene mit Knieosteoarthritis
Arthrosamid® ist ein nicht resorbierbares, nicht biologisch abbaubares, injizierbares, transparentes, hydrophiles Gel, bestehend aus einem Grundgerüst aus fest gebundenem, nicht biologisch abbaubarem Polyacrylamid (2,5 %) und daran gebundenem nicht-pyrogenem Wasser (97,5 %)
Arthrosamid® wird als vorgefüllte, sterile 1-ml-Spritze zum einmaligen Gebrauch geliefert, die mit einem Luer-Lock-Anschluss und einer Verschlusskappe verschlossen ist. Es ist für die intraartikuläre Injektion in das Kniegelenk mit einer sterilen 21G x 2 Zoll (0,8 x 50 mm) Nadel vorgesehen.
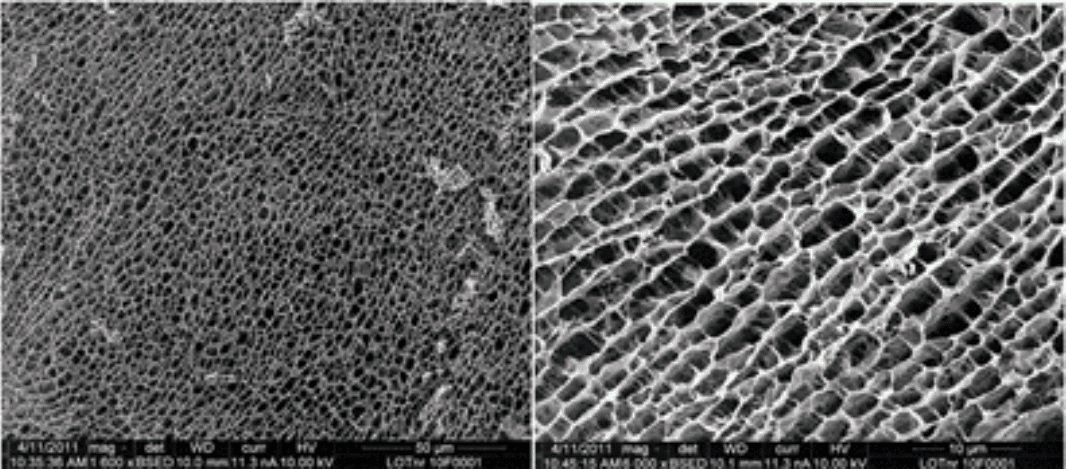
Abbildung 1 zeigt die dreidimensionale Struktur des Polyacrylamid-Hydrogels. Die dichte, gleichmäßige Wabenstruktur bietet eine Matrix für das Einwachsen von Zellen.
Chemische Beschreibung von Polyacrylamid
Wie oben beschrieben, besteht das Arthrosamid® Hydrogel aus 2,5 % vernetztem Polyacrylamid in der Trockenmasse und 97,5 % nicht-pyrogenem Wasser. Während der Synthese polymerisiert N,N-Methylen-bis-Acrylamid mit Acrylamid, wodurch Vernetzungen zwischen den Polyacrylamidketten entstehen.
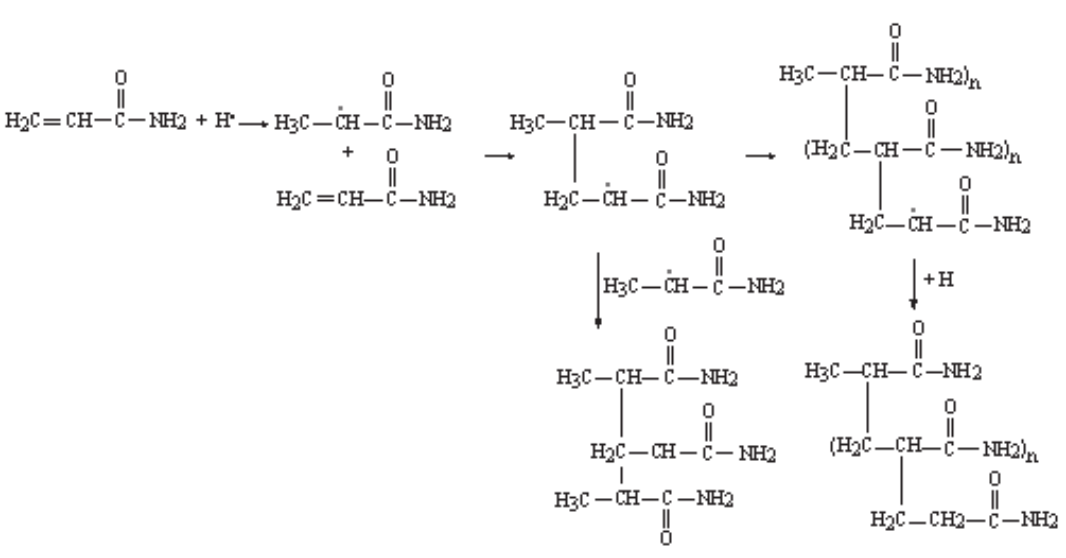
Das vernetzte Polyacrylamid-Hydrogel wird in einem Polymerisationsverfahren synthetisiert, bei dem sich wiederholende Acrylamid-Einheiten in einer Kettenreaktion miteinander verbunden werden.
Die Kettenreaktion beruht auf einem Redox-Initiator-Prinzip, bei dem ein Ammoniumpersulfat (AMPS)-Initiator ein freies Radikal erzeugt, das sich an ein Acrylamid-Monomer anlagert, indem es ein Elektron aus der Doppelbindung im Acrylamid gewinnt und so eine Kohlenstoff-Kohlenstoff-Einfachbindung mit dem Acrylamid bildet. Dadurch bleibt ein nicht geteiltes Elektron für die weitere Anlagerung von Acrylamidmonomeren übrig, wie in Abbildung 2 rechts dargestellt.
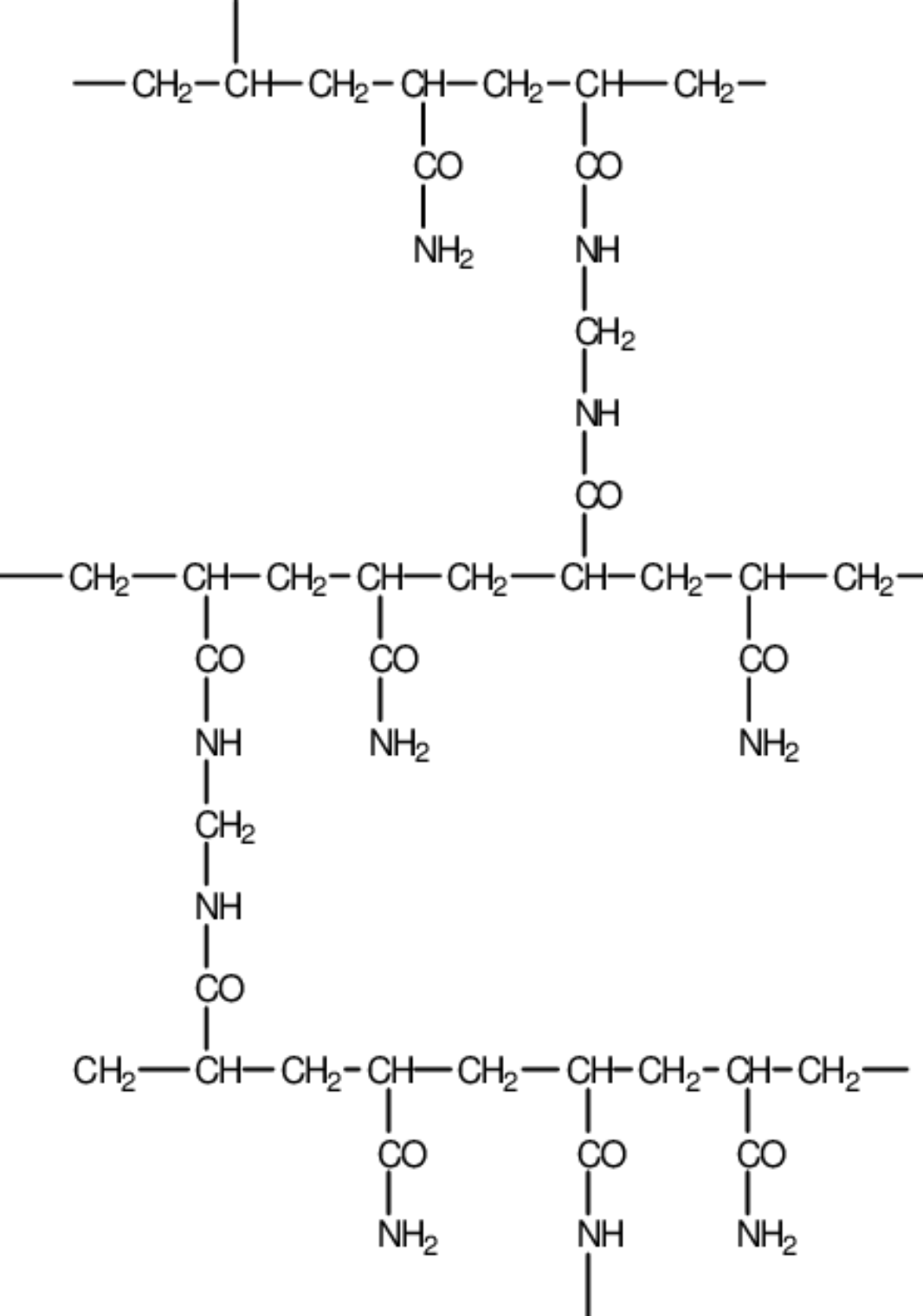
Die Verzweigung des linearen Kohlenstoff-Kohlenstoff-Grundgerüsts von Polyacrylamid erfolgt durch das Vorhandensein eines Vernetzungsmittels, des N,N-Methylen-bis-Acrylamid-Monomers (MBAM), wie in Abbildung 3 dargestellt.
Nach der Verzweigung der Polyacrylamid-Hauptketten bildet sich ein dreidimensionales Netz aus vernetztem Polyacrylamid anstelle von unverbundenen linearen Polyacrylamidketten.
Arthrosamid® Materialien und Biokompatibilität
Arthrosamid® enthält keine Arzneimittel, Gewebe oder Blutprodukte.
Die in Arthrosamid® verwendeten Materialien sind nachstehend aufgeführt (Tabelle 2).
Geräteteil |
Material |
Körperkontakt |
|
|---|---|---|---|
Gel |
Hydrophiles Gel, bestehend aus etwa 2,5 % vernetztem Polyacrylamid und 97,5 % nicht-pyrogenem Wasser |
Kniegelenk |
|
Spritze |
Zylinder |
Polypropylen |
Haut* |
Kolben |
Polycarbonat |
Haut* |
|
Gummistopfen |
Silikongummi |
Haut* |
|
Schmiermittel |
Silikonöl |
Haut* |
|
Verschlusskappe |
Polypropylen |
Haut* |
|
Tabelle 2. Materialien des Geräts. *Die Spritze wird vom Benutzer gehandhabt, der Schutzhandschuhe tragen sollte. Daher sollten normalerweise weder der Patient noch der Anwender mit der Spritze in Berührung kommen. Der Gummistopfen und das Schmiermittel sind nicht exponiert, so dass das Risiko, mit ihnen in Kontakt zu kommen, noch geringer ist als bei den exponierten Spritzenteilen.
Die Biokompatibilitätstests wurden gemäß ISO 10993-1 für die bestehenden Hydrogelprodukte von Contura durchgeführt. Die Tests, die für Arthrosamid® als relevant erachtet werden, sind im Folgenden zusammengefasst (Tabelle 3) und im Biological Evaluation Report (BER) – Arthrosamid® ausführlich beschrieben.
Endpunkt der biologischen Bewertung |
Standard-Referenz |
Test und Testnummer |
Datum des Berichts |
Ergebnis |
|---|---|---|---|---|
Zytotoxizität |
ISO 10993-5:2009 USP 29 |
Hydrogel B: In-vitro-Zytotoxizitätstest Nr. 16/368-030C |
2017 |
Pass |
Sensibilisierung |
ISO 10993-10: 2010 |
Bewertung der Kontaktüberempfindlichkeit beim Meerschweinchen (Maximierungstest) Lokale Lymphknotenuntersuchung bei Mäusen Nr. 517557 |
2017 |
Pass |
Hydrogel B: Lokaler Lymphknoten-Assay (Hautsensibilisierung) Nr. 77691) |
2017 |
|||
Irritation oder intrakutane Reaktivität |
ISO 10993-10: 2010 |
Intrakutaner Reaktivitätstest am Kaninchen Nr. 77693 |
2017 |
Pass |
Systemische Toxizität (akut) |
ISO 10993-11: 2017 / 10993-12: 2012 USP 151 |
Materialvermittelter Pyrogenitätstest Nr. APS-GZJ009-ST01 |
2018 |
Pass |
Subchronische Toxizität (subakute Toxizität) |
ISO 10993-6:2007 |
Systemische Toxizitätsendpunkte für die subchronische Toxizität wurden in der Zwei-Jahres-Implantationsstudie an Schafen untersucht Nr. 285465 |
2017 |
Pass |
Genotoxizität |
ISO 10993-3: 2014 |
Bakterieller Umkehrmutationstest (Ames-Test) Nr. 16/368-007M |
2017 |
Pass |
In vitro-Test auf Chromosomenaberrationen bei Säugetieren Nr. 16/368-020C |
2017 |
|||
In vivo Säugetier-Erythrozyten-Mikronukleustest Nr. 16/368-013E |
2017 APR07 |
|||
Implantation |
ISO 10993-6:2007 |
Zwei-Jahres-Implantationsstudie bei Schafen Nr. 285465 |
2017 |
Pass |
Tabelle 3. Biokompatibilitätsstudien (und Implantationsstudie) für das Hydrogel von Contura
Aufgrund der durchgeführten Tests gilt Arthrosamid® als biokompatibel und für den langfristigen Kontakt mit dem Körper geeignet.
Stabilität und Lebensdauer von Arthrosamid®
Die Stabilität der Polyacrylamid-Hydrogele von Contura wird im Biological Evaluation Report (BER) – Arthrosamid®ausführlich beschrieben und erörtert, und eine Zusammenfassung der Stabilitätstests zur Untersuchung der potenziellen Hydrolyse, oxidativen und physikalischen Belastung von „Hydrogel B“ ist nachstehend aufgeführt (Tabelle 5). Wie in der GVO dargelegt, wurde der enzymatische Abbau von Polyacrylamid in verschiedenen enzymatischen Fermentationssystemen getestet, wobei jedoch kein Abbau beobachtet wurde.
| Zustand | Test | Ergebnis | Test-Referenz |
|---|---|---|---|
| Hydrolyse und oxidativer Stress | Doppelte Hydrogel B-Proben wurden 24 Stunden bei 37 °C in nicht-oxidativen, mäßig oxidativen und extrem oxidativen hypotonischen und isotonischen Lösungsmitteln inkubiert. pH 2-eingestellte und nicht eingestellte neutrale Lösungsmittel wurden verglichen. Die Proben wurden mittels HPLC analysiert. | Hydrogel B zeigte keine Tendenz zur Bildung von monomerem Acrylamid unter nicht-oxidativen, oxidativen und aggressiven hydrolytischen, sauren Testbedingungen. | ChemPilot 2018 |
| Physischer Stress | In einem Versuchsaufbau wurde das Hydrogel einer extremen mechanischen Scherbeanspruchung in einem Messermischverfahren ausgesetzt. | Extreme mechanische Belastungen führten nicht zu einem Abbau des Hydrogels in Acrylamidmonomere. Extreme mechanische Beanspruchung, wie sie bei der Messermischung auftritt, findet unter physiologischen Bedingungen nicht statt. | Contura (011.INR.00025) |
Tabelle 5. Mit dem Hydrogel von Contura („Hydrogel B“) durchgeführte Stabilitätsstudien.
Es zeigt sich, dass das Polyacrylamid-Hydrogel stabil ist und sich unter den Testbedingungen nicht abbaut.
Arthrosamid® Stabilität – Migration
Das Migrationspotenzial des Polyacrylamid-Hydrogels wurde umfassend untersucht, wie im BER und im Bericht „Evaluation of Arthrosamid® Migration and Degradation Potential After Intraarticular Administration“ dargelegt. Kurz gesagt, wurde in Bezug auf die intraartikuläre Injektion beobachtet, dass kleine Partikel (8 µm oder weniger) der Phagozytose unterliegen und mit der Synovialflüssigkeit durch die Gap Junctions im Synovialepithel fließen und schließlich systemisch verteilt werden, während größere Partikel (> 8–17 µm) mit der Zeit eingekapselt werden und auf unbestimmte Zeit im Weichteilgewebe immobilisiert bleiben. Wie bereits beschrieben, wird Arthrosamid®/„Hydrogel“ als vernetzte Matrix aus Polyacrylamidketten gebildet. Das endgültige Material, so wie es injiziert wird, hat im Wesentlichen keine kleinen Partikelkomponenten, und die kleinste messbare Partikelgröße wurde mit > 300 μm gemessen, was weit über der Partikelgröße von nur einem Mikrometer liegt, die als physiologisch mobil beschrieben wurde.
In Studien an Kaninchen und Pferden wurden Makrophagen und Riesenzellen beobachtet, die mit dem Hydrogel assoziiert waren, und es gab keine Hinweise auf Hydrogelpartikel in Phagosomen in diesen Zellen (Christensen et al., 2016). Es wurden weitere Studien durchgeführt, in denen drainierende Lymphknoten und Gewebe in der Nähe von Weichteilinjektionsstellen untersucht wurden, wobei kein Nachweis von Hydrogel in den lokalen drainierenden Lymphknoten oder in entfernten Organen erbracht wurde (Charles River, 2011). Das Migrationspotenzial der Polyacrylamid-Hydrogele von Contura wird in dem BER ausführlich beschrieben und erörtert, wobei – auf der Grundlage der veröffentlichten Literatur und der spezifischen Tests von Arthrosamid® – der Schluss gezogen wird, dass das Polyacrylamid-Hydrogel als dauerhaftes Implantat im subsynovialen Gewebe verbleibt.
Arthrosamid® – Klinische und präklinische Nachweise für iPAAG
Bei Kaninchen und Pferden wurde die Integration des Hydrogels bis zu zwei Jahre nach der Injektion verfolgt. Bei Pferden erschien das Hydrogel zwei Wochen nach der Behandlung als innere Schicht in der Synovialschleimhaut, die mit proliferierenden Synovialzellen durchsetzt war, ähnlich der Histologie im Kaninchenmodell. Nach einem Monat hatten sich die Synovialzellen offenbar an die Oberfläche verlagert, und nach 3, 8 und 24 Monaten wurde ein ähnliches Muster der Integration beobachtet (Christensen et al., 2016). Das Hydrogel war als integrierte Zone im subsynovialen Interstitium mit einem feinen gefäßtragenden Gewebenetz und sehr wenigen Entzündungszellen vorhanden.
In einer prospektiven histopathologischen Studie wurde Gewebe untersucht, das Patienten im Rahmen einer Knie-Totalendoprothese (TKA) entnommen wurde. Die Patienten waren 5–33 Monate zuvor mit dem Hydrogel behandelt worden. In allen sieben Fällen wurde ein ähnliches histologisches Muster festgestellt: Es stellte sich heraus, dass das Hydrogel in die Synovialmembran integriert war und äußere Synovialschleimhautzellen in das Gel eingedrungen waren und eine neue Schleimschicht gebildet hatten. Ein ähnliches Muster wurde 9 Monate nach einer TKA in einer Fallstudie beschrieben (Christensen und Daugaard, 2016).
Die Hydrogele von Contura werden seit 2001 vermarktet, und es wurde eine Reihe von klinischen Studien mit unterschiedlichen Nachbeobachtungszeiten für verschiedene Indikationen durchgeführt. Langzeitdaten über das Contura-Polyacrylamid-Hydrogel liegen aus einer 10-Jahres-Follow-up-Studie vor, an der 104 HIV-Patienten teilnahmen, denen durchschnittlich 6 ml Aquamid®-Hydrogel zur Behandlung von Lipothrophie im Gesicht injiziert wurde. Bei der Nachuntersuchung (10 Jahre) wies kein Patient eine Migration des Hydrogels auf und die Mehrheit der Patienten war mit dem kosmetischen Ergebnis „sehr zufrieden“ (74,8 %) oder „zufrieden“ (23,4 %) (Negredo et al., 2015). Ein stabiles Erscheinungsbild des Hydrogels wurde auch in einer achtjährigen Nachfolgestudie an 25 Frauen mit Belastungsharninkontinenz beobachtet, die mit Bulkamid®-Hydrogel behandelt worden waren, wobei alle Patientinnen sichtbare Polyacrylamid-Hydrogel-Ablagerungen im vaginalen Ultraschall hatten (Mouritsen et al., 2014).
Schlussfolgerung – Stabilität und Lebensdauer von Arthrosamid®
Wie in diesem und den vorhergehenden Abschnitten beschrieben, haben präklinische Studien gezeigt, dass Arthrosamid®/„Hydrogel“ biokompatibel, nicht resorbierbar, nicht biologisch abbaubar und nicht migrierend ist (Bello et al., 2007; Charles River, 2011; Zarini et al., 2004). Langfristige klinische Daten haben dies bestätigt (Mouritsen et al., 2014; Negredo et al., 2015). Daher kann man davon ausgehen, dass Arthrosamid® während der gesamten Lebensdauer des Geräts stabil und sicher ist.
Der Verwendungszweck von Arthrosamid® ist im Folgenden zusammengefasst:
Verwendungszweck von Arthrosamid® |
|
Indikation |
Arthrosamid® ist für die symptomatische Behandlung erwachsener Patienten mit Knieosteoarthritis geeignet. |
Zu behandelnde Krankheit |
Knieosteoarthritis. |
Patientenpopulation |
Erwachsene Patienten mit diagnostizierter Osteoarthritis. |
Verwendungszweck |
Arthrosamid® ist für die intraartikuläre Injektion in das Kniegelenk bestimmt. |
Beabsichtigter Benutzer |
Arthrosamid® ist für die Anwendung durch einen qualifizierten Arzt bestimmt, der mit intraartikulären Injektionsverfahren vertraut ist, wie z. B. orthopädische Chirurgen oder Rheumatologen. |
Wirkung auf den menschlichen Körper |
Arthrosamid® lindert die Schmerzen und verbessert die Funktion des von Osteoarthritis betroffenen Knies. |
Gewebe in Kontakt mit dem Produkt |
Kniegelenk. |
Dauer der Nutzung |
Langfristig (>30 Tage)*. |
Kontakt mit Schleimhäuten |
Arthrosamid® ist in Kontakt mit der Synovialmembran des Kniegelenks. |
Invasiv / nicht-invasiv |
Invasiv. |
Implantierbar / nicht-implantierbar |
Implantierbar. |
Einmalig / wiederverwendbar |
Einmaliger Gebrauch. |
Empfohlene Dosis |
6 ml**. |
Kontraindikationen |
Arthrosamid® darf nicht gespritzt werden:
|
Warnungen |
|
Vom Hersteller vorgeschriebene Vorsichtsmaßnahmen |
|
Tabelle 6. Verwendungszweck von Arthrosamid®. *Für Arthrosamid® werden klinische Nachbeobachtungsdaten von zwölf Monaten vorgelegt (siehe 5.4.1 und 5.4.4), während für die Hydrogele von Contura für andere Indikationen klinische Langzeitdaten von bis zu 8 oder 10 Jahren vorliegen (3.1.2.10), sodass davon ausgegangen werden kann, dass dieses Dauerimplantat/Hydrogel während der gesamten Lebensdauer des Produkts stabil und sicher ist (3.1.2.10).
**Die empfohlene Dosierung von 6 ml basiert auf der Gesamtmenge des in der „Proof-of-Concept“-Studie injizierten Gels (2 x 3 ml für die Mehrheit (96 %) der Patienten) und auf Daten aus der CON-OA-Studie (5.4.4). Eine Injektion von 6 ml im Vergleich zu 2 x 3 ml verringert das Infektionsrisiko, und die prophylaktischen Antibiotika werden nur einmal verabreicht.

Möchten Sie Arthrosamid® verwenden?
Sichere und nachhaltige Schmerzlinderung mit einer einzigen Injektion. Kontaktieren Sie uns, um Arthrosamid® iPAAG noch heute bei Ihren Patienten mit Knieosteoarthritis einzusetzen.
References
Alhede, M., Er, O., Eickhardt, S., Kragh, K., Alhede, M., Christensen, L.D., Poulsen, S.S., Givskov, M., Christensen, L.H., Hoiby, N., Tvede, M., Bjarnsholt, T., 2014. Bacterial biofilm formation and treatment in soft tissue fillers. Pathogens and disease 70, 339-346.
Altman, D., Ghilotti, F., Bellocco, R., Zetterstrom, J., Kopp Kallner, H., 2017. Transurethral Polyacrylamide Hydrogel Injection Therapy in Women Not Eligible for Midurethral Sling Surgery. Female pelvic medicine & reconstructive surgery 23, 318-323.
Altman, D., Hjern, F., Zetterstrom, J., 2016a. Transanal submucosal polyacrylamide gel injection treatment of anal incontinence: a randomized controlled trial. Acta Obstet Gynecol Scand 95, 528-533.
Altman, R.D., Bedi, A., Karlsson, J., Sancheti, P., Schemitsch, E., 2016b. Product Differences in Intra-articular Hyaluronic Acids for Osteoarthritis of the Knee. The American journal of sports medicine 44, 2158-2165.
Bagga, H., Burkhardt, D., Sambrook, P., March, L., 2006. Longterm effects of intraarticular hyaluronan on synovial fluid in osteoarthritis of the knee. J Rheumatol 33, 946-950.
Balazs, E.A., 2004. Viscosupplementation for treatment of osteoarthritis: from initial discovery to current status and results. Surgical technology international 12, 278-289.
Bellamy, N., Campbell, J., Robinson, V., Gee, T., Bourne, R., Wells, G., 2006. Viscosupplementation for the treatment of osteoarthritis of the knee. The Cochrane database of systematic reviews, Cd005321.
Bellamy, N., Hochberg, M., Tubach, F., Martin-Mola, E., Awada, H., Bombardier, C., Hajjaj-Hassouni, N., Logeart, I., Matucci-Cerinic, M., van de Laar, M., van der Heijde, D., Dougados, M., 2015. Development of multinational definitions of minimal clinically important improvement and patient acceptable symptomatic state in osteoarthritis. Arthritis care & research 67, 972-980.
Bello, G., Jackson, I.T., Keskin, M., Kelly, C., Dajani, K., Studinger, R., Kim, E., Lincoln, D., Silberberg, B., Lee, A., 2007. The Use of Polyacrylamide Gel in Soft Tissue Augmentation: An Experimental Assessment. Plast.Reconstr.Surg 119, 1326-1336.
Belluzzi, E., Stocco, E., Pozzuoli, A., Granzotto, M., Porzionato, A., Vettor, R., De Caro, R., Ruggieri, P., Ramonda, R., Rossato, M., Favero, M., Macchi, V., 2019. Contribution of Infrapatellar Fat Pad and Synovial Membrane to Knee Osteoarthritis Pain. Biomed Res Int 2019, 6390182.
Belmont, P.J., Jr., Goodman, G.P., Waterman, B.R., Bader, J.O., Schoenfeld, A.J., 2014. Thirty-day postoperative complications and mortality following total knee arthroplasty: incidence and risk factors among a national sample of 15,321 patients. The Journal of bone and joint surgery. American volume 96, 20-26.
Benazzo, F., Perticarini, L., Padolino, A., Castelli, A., Gifuni, P., Lovato, M., Manzini, C., Giordan, N., 2016. A multi-centre, open label, long-term follow-up study to evaluate the benefits of a new viscoelastic hydrogel (Hymovis(R)) in the treatment of knee osteoarthritis. European review for medical and pharmacological sciences 20, 959-968.
Bisicchia, S., Bernardi, G., Tudisco, C., 2016. HYADD 4 versus methylprednisolone acetate in symptomatic knee osteoarthritis: a single-centre single blind prospective randomised controlled clinical study with 1-year follow-up. Clinical and experimental rheumatology 34, 857-863.
Bruyere, O., Cooper, C., Pelletier, J.P., Maheu, E., Rannou, F., Branco, J., Luisa Brandi, M., Kanis, J.A., Altman, R.D., Hochberg, M.C., Martel-Pelletier, J., Reginster, J.Y., 2016. A consensus statement on the European Society for Clinical and Economic Aspects of Osteoporosis and Osteoarthritis (ESCEO) algorithm for the management of knee osteoarthritis-From evidence-based medicine to the real-life setting. Seminars in arthritis and rheumatism 45, S3-11.
Bruyere, O., Honvo, G., Veronese, N., Arden, N.K., Branco, J., Curtis, E.M., Al-Daghri, N.M., Herrero-Beaumont, G., Martel-Pelletier, J., Pelletier, J.P., Rannou, F., Rizzoli, R., Roth, R., Uebelhart, D., Cooper, C., Reginster, J.Y., 2019. An updated algorithm recommendation for the management of knee osteoarthritis from the European Society for Clinical and Economic Aspects of Osteoporosis, Osteoarthritis and Musculoskeletal Diseases (ESCEO). Seminars in arthritis and rheumatism 49, 337-350.
Carr, A.J., Robertsson, O., Graves, S., Price, A.J., Arden, N.K., Judge, A., Beard, D.J., 2012. Knee replacement. Lancet 379, 1331-1340.
Charles River 2011. Assessment of local and systemic effects of Bulkamid hydrogel for urethral implantation - a two year follow-up study in sheep. Study No 285465.
Chempilots 2004. Description of the gel's chemical/physical structure, 1-3.
Christensen, L., 2007. Normal and pathologic tissue reactions to soft tissue gel fillers. Dermatol.Surg. 33 Suppl 2, S168-S175.
Christensen, L. 2019. The synovium – interaction with gel endoprosthesis – clinical outcome in OA (unpublished).
Christensen, L., Breiting, V., Bjarnsholt, T., Eickhardt, S., Hogdall, E., Janssen, M., Pallua, N., Zaat, S.A., 2013. Bacterial infection as a likely cause of adverse reactions to polyacrylamide hydrogel fillers in cosmetic surgery. Clinical infectious diseases : an official publication of the Infectious Diseases Society of America 56, 1438-1444.
Christensen, L., Camitz, L., Illigen, K.E., Hansen, M., Sarvaa, R., Conaghan, P.G., 2016. Synovial incorporation of polyacrylamide hydrogel after injection into normal and osteoarthritic animal joints. Osteoarthritis and cartilage / OARS, Osteoarthritis Research Society 24, 1999-2002.
Christensen, L., Daugaard, S., 2016. Histological Appearance of the Synovial Membrane after Treatment of Knee Osteoarthritis with Polyacrylamide Gel Injections: A Case Report. Journal of Arthritis 5, 217.
Christensen, L.H., 2009. Host tissue interaction, fate, and risks of degradable and nondegradable gel fillers. Dermatol.Surg. 35 Suppl 2, 1612-1619.
Christensen, L.H., Nielsen, J.B., Mouritsen, L., Sorensen, M., Lose, G., 2008. Tissue integration of polyacrylamide hydrogel: an experimental study of periurethral, perivesical, and mammary gland tissue in the pig. Dermatol.Surg. 34 Suppl 1, S68-S77.
de Clifford, L.T., Lowe, J.N., McKellar, C.D., Bolwell, C., David, F., 2019. Use of a 2.5% Cross-Linked Polyacrylamide Hydrogel in the Management of Joint Lameness in a Population of Flat Racing Thoroughbreds: A Pilot Study. Journal of Equine Veterinary Science 77, 57-62.
De Santis, G., Pignatti, M., Baccarani, A., Pedone, A., Spaggiari, A., Orlando, G., Guaraldi, G., 2012. Long-term efficacy and safety of polyacrylamide hydrogel injection in the treatment of human immunodeficiency virus-related facial lipoatrophy: a 5-year follow-up. Plast Reconstr Surg 129, 101-109.
Di Matteo, B., Vandenbulcke, F., Vitale, N.D., Iacono, F., Ashmore, K., Marcacci, M., Kon, E., 2019. Minimally Manipulated Mesenchymal Stem Cells for the Treatment of Knee Osteoarthritis: A Systematic Review of Clinical Evidence. Stem cells international 2019, 1735242.
Divine, J.G., Zazulak, B.T., Hewett, T.E., 2006. Viscosupplementation for knee osteoarthritis: a systematic review. Clinical orthopaedics and related research 455, 113-122.
Fam, H., Bryant, J.T., Kontopoulou, M., 2007. Rheological properties of synovial fluids. Biorheology 44, 59-74.
Faundez, E., Vega, N., Vera, E., Vega, P., Sepulveda, D., Wortsman, X., 2017. Clinical and color Doppler ultrasound evaluation of polyacrylamide injection in HIV patients with severe facial lipoatrophy secondary to antiretroviral therapy. Skin research and technology : official journal of International Society for Bioengineering and the Skin (ISBS) [and] International Society for Digital Imaging of Skin (ISDIS) [and] International Society for Skin Imaging (ISSI) 23, 243-248.
Felson, D.T., Lawrence, R.C., Dieppe, P.A., Hirsch, R., Helmick, C.G., Jordan, J.M., Kington, R.S., Lane, N.E., Nevitt, M.C., Zhang, Y., Sowers, M., McAlindon, T., Spector, T.D., Poole, A.R., Yanovski, S.Z., Ateshian, G., Sharma, L., Buckwalter, J.A., Brandt, K.D., Fries, J.F., 2000. Osteoarthritis: new insights. Part 1: the disease and its risk factors. Annals of internal medicine 133, 635-646.
Goldman, D.T., Piechowiak, R., Nissman, D., Bagla, S., Isaacson, A., 2018. Current Concepts and Future Directions of Minimally Invasive Treatment for Knee Pain. Current rheumatology reports 20, 54.
Gomis, A., Pawlak, M., Balazs, E.A., Schmidt, R.F., Belmonte, C., 2004. Effects of different molecular weight elastoviscous hyaluronan solutions on articular nociceptive afferents. Arthritis and rheumatism 50, 314-326.
Hansen, M.F., Lose, G., Kesmodel, U.S., Gradel, K.O., 2017. A national population-based cohort study of urethral injection therapy for female stress and mixed urinary incontinence: the Danish Urogynaecological Database, 2007-2011. Int Urogynecol J, doi: 10.1007/s00192-00017-03265-z.
Hartkopp, A. 2015. Injection of non-degradable polyacrylamide gel into the knee joint has long-term effect on osteoarthritis symptoms – a pilot study (A2 Clinic of Rheumatology and Sports Medicine A/S, Hillerød, Denmark).
He, W.W., Kuang, M.J., Zhao, J., Sun, L., Lu, B., Wang, Y., Ma, J.X., Ma, X.L., 2017. Efficacy and safety of intraarticular hyaluronic acid and corticosteroid for knee osteoarthritis: A meta-analysis. International journal of surgery (London, England) 39, 95-103.
Henriksen, M., Overgaard, A., Hartkopp, A., Bliddal, H., 2018. Intra-articular 2.5% polyacrylamide hydrogel for the treatment of knee osteoarthritis: an observational proof-of-concept cohort study. Clinical and experimental rheumatology 36, 1082-1085.
Hermans, J., Bierma-Zeinstra, S.M.A., Bos, P.K., Niesten, D.D., Verhaar, J.A.N., Reijman, M., 2019. The effectiveness of high molecular weight hyaluronic acid for knee osteoarthritis in patients in the working age: a randomised controlled trial. BMC musculoskeletal disorders 20, 196.
Hochberg, M.C., Altman, R.D., April, K.T., Benkhalti, M., Guyatt, G., McGowan, J., Towheed, T., Welch, V., Wells, G., Tugwell, P., 2012. American College of Rheumatology 2012 recommendations for the use of nonpharmacologic and pharmacologic therapies in osteoarthritis of the hand, hip, and knee. Arthritis care & research 64, 465-474.
Hollenz, M., Stolte, M., Leodolter, A., Labenz, J., 2006. NSAID-associated dyspepsia and ulcers: a prospective cohort study in primary care. Digestive diseases (Basel, Switzerland) 24, 189-194.
Hootman, J.M., Helmick, C.G., 2006. Projections of US prevalence of arthritis and associated activity limitations. Arthritis and rheumatism 54, 226-229.
Itkonen Freitas, A.M., Mentula, M., Rahkola-Soisalo, P., Tulokas, S., Mikkola, T.S., 2020. Tension-Free Vaginal Tape Surgery versus Polyacrylamide Hydrogel Injection for Primary Stress Urinary Incontinence: A Randomized Clinical Trial. J Urol 203, 372-378.
Jette, D.U., Hunter, S.J., Burkett, L., Langham, B., Logerstedt, D.S., Piuzzi, N.S., Poirier, N.M., Radach, L.J.L., Ritter, J.E., Scalzitti, D.A., Stevens-Lapsley, J.E., Tompkins, J., Zeni, J., Jr., 2020. Physical Therapist Management of Total Knee Arthroplasty. Phys Ther 100, 1603-1631.
Jevsevar, D., Donnelly, P., Brown, G.A., Cummins, D.S., 2015. Viscosupplementation for Osteoarthritis of the Knee: A Systematic Review of the Evidence. The Journal of bone and joint surgery. American volume 97, 2047-2060.
Jevsevar, D.S., Brown, G.A., Jones, D.L., Matzkin, E.G., Manner, P.A., Mooar, P., Schousboe, J.T., Stovitz, S., Sanders, J.O., Bozic, K.J., Goldberg, M.J., Martin, W.R., 3rd, Cummins, D.S., Donnelly, P., Woznica, A., Gross, L., 2013. The American Academy of Orthopaedic Surgeons evidence-based guideline on: treatment of osteoarthritis of the knee, 2nd edition. https://www.aaos.org/research/guidelines/treatmentofosteoarthritisofthekneeguideline.pdf. The Journal of bone and joint surgery. American volume 95, 1885-1886.
Kasi, A.D., Pergialiotis, V., Perrea, D.N., Khunda, A., Doumouchtsis, S.K., 2016. Polyacrylamide hydrogel (Bulkamid(R)) for stress urinary incontinence in women: a systematic review of the literature. Int Urogynecol J 27, 367-375.
Kohn, M.D., Sassoon, A.A., Fernando, N.D., 2016. Classifications in Brief: Kellgren-Lawrence Classification of Osteoarthritis. Clinical orthopaedics and related research 474, 1886-1893.
Kolasinski, S.L., Neogi, T., Hochberg, M.C., Oatis, C., Guyatt, G., Block, J., Callahan, L., Copenhaver, C., Dodge, C., Felson, D., Gellar, K., Harvey, W.F., Hawker, G., Herzig, E., Kwoh, C.K., Nelson, A.E., Samuels, J., Scanzello, C., White, D., Wise, B., Altman, R.D., DiRenzo, D., Fontanarosa, J., Giradi, G., Ishimori, M., Misra, D., Shah, A.A., Shmagel, A.K., Thoma, L.M., Turgunbaev, M., Turner, A.S., Reston, J., 2020. 2019 American College of Rheumatology/Arthritis Foundation Guideline for the Management of Osteoarthritis of the Hand, Hip, and Knee. Arthritis care & research 72, 149-162.
Krhut, J., Martan, A., Jurakova, M., Nemec, D., Masata, J., Zvara, P., 2016. Treatment of stress urinary incontinence using polyacrylamide hydrogel in women after radiotherapy: 1-year follow-up. Int Urogynecol J 27, 301-305.
Langworthy, M.J., Saad, A., Langworthy, N.M., 2010. Conservative treatment modalities and outcomes for osteoarthritis: the concomitant pyramid of treatment. The Physician and sportsmedicine 38, 133-145.
Leighton, R., Akermark, C., Therrien, R., Richardson, J.B., Andersson, M., Todman, M.G., Arden, N.K., 2014. NASHA hyaluronic acid vs. methylprednisolone for knee osteoarthritis: a prospective, multi-centre, randomized, non-inferiority trial. Osteoarthritis and cartilage / OARS, Osteoarthritis Research Society 22, 17-25.
Leighton, R., Fitzpatrick, J., Smith, H., Crandall, D., Flannery, C.R., Conrozier, T., 2018. Systematic clinical evidence review of NASHA (Durolane hyaluronic acid) for the treatment of knee osteoarthritis. Open Access Rheumatol 10, 43-54.
Leone Roberti Maggiore, U., Alessandri, F., Medica, M., Gabelli, M., Venturini, P.L., Ferrero, S., 2013. Outpatient periurethral injections of polyacrylamide hydrogel for the treatment of female stress urinary incontinence: effectiveness and safety. Archives of gynecology and obstetrics 288, 131-137.
Liddle, A.D., Judge, A., Pandit, H., Murray, D.W., 2014. Adverse outcomes after total and unicompartmental knee replacement in 101,330 matched patients: a study of data from the National Joint Registry for England and Wales. Lancet 384, 1437-1445.
Lowe, J.N., de Clifford, L., McKellar, K., 2016. Intra-articular 2.5% Polyacrylamide Hydrogel (PAAG) for the Treatment of Osteoarthritis in 54 Thoroughbred Racehorses: A Prospective Study. Poster presented at the 38th Bain Fallon Memorial Lectures, Melbourne, Australia run by the Equine Veterinarians Australia, the special interest branch of the Australian Veterinary Association.
Maheu, E., Bannuru, R.R., Herrero-Beaumont, G., Allali, F., Bard, H., Migliore, A., 2019. Why we should definitely include intra-articular hyaluronic acid as a therapeutic option in the management of knee osteoarthritis: Results of an extensive critical literature review. Seminars in arthritis and rheumatism 48, 563-572.
Maheu, E., Rannou, F., Reginster, J.Y., 2016. Efficacy and safety of hyaluronic acid in the management of osteoarthritis: Evidence from real-life setting trials and surveys. Seminars in arthritis and rheumatism 45, S28-33.
Marsland, D., Mumith, A., Barlow, I.W., 2014. Systematic review: the safety of intra-articular corticosteroid injection prior to total knee arthroplasty. The Knee 21, 6-11.
Martan, A., Masata, J., Svabik, K., Krhut, J., 2014. Transurethral injection of polyacrylamide hydrogel (Bulkamid((R))) for the treatment of female stress or mixed urinary incontinence. European journal of obstetrics, gynecology, and reproductive biology 178, 199-202.
Mathiessen, A., Conaghan, P.G., 2017. Synovitis in osteoarthritis: current understanding with therapeutic implications. Arthritis research & therapy 19, 18.
McAlindon, T.E., Bannuru, R.R., Sullivan, M.C., Arden, N.K., Berenbaum, F., Bierma-Zeinstra, S.M., Hawker, G.A., Henrotin, Y., Hunter, D.J., Kawaguchi, H., Kwoh, K., Lohmander, S., Rannou, F., Roos, E.M., Underwood, M., 2014. OARSI guidelines for the non-surgical management of knee osteoarthritis. Osteoarthritis and cartilage / OARS, Osteoarthritis Research Society 22, 363-388.
McGrory, B.J., Weber, K.L., Jevsevar, D.S., Sevarino, K., 2016. Surgical Management of Osteoarthritis of the Knee: Evidence-based Guideline. The Journal of the American Academy of Orthopaedic Surgeons 24, e87-93.
Miller, L.E., Block, J.E., 2013. US-Approved Intra-Articular Hyaluronic Acid Injections are Safe and Effective in Patients with Knee Osteoarthritis: Systematic Review and Meta-Analysis of Randomized, Saline-Controlled Trials. Clinical medicine insights. Arthritis and musculoskeletal disorders 6, 57-63.
Mohr, S., Marthaler, C., Imboden, S., Monga, A., Mueller, M.D., Kuhn, A., 2017. Bulkamid (PAHG) in mixed urinary incontinence: What is the outcome? Int Urogynecol J 28, 1657-1661.
Mohr, S., Siegenthaler, M., Mueller, M.D., Kuhn, A., 2013. Bulking agents: an analysis of 500 cases and review of the literature. Int Urogynecol J 24, 241-247.
Mouritsen, L., Lose, G., Moller-Bek, K., 2014. Long-term follow-up after urethral injection with polyacrylamide hydrogel for female stress incontinence. Acta Obstet Gynecol Scand 93, 209-212.
National Clinical Guideline Centre. 2014. National Institute for Health and Clinical Excellence: Guidance. https://www.ncbi.nlm.nih.gov/books/NBK248069/pdf/Bookshelf_NBK248069.pdf, In: Osteoarthritis: Care and Management in Adults. National Institute for Health and Care Excellence (UK), National Clinical Guideline Centre, 2014., London.
Negredo, E., Puig, J., Ornelas, A., Echeverria, P., Bonjoch, A., Estany, C., Higueras, C., Gonzalez-Mestre, V., Clotet, B., 2015. Ten-Year Safety with Polyacrylamide Gel Used to Correct Facial Lipoatrophy in HIV-Infected Patients. AIDS Res Hum Retroviruses 31, 817-821.
Overgaard, A., Bliddal, H., Henriksen, M., 2019. Safety of Intra-Articular Polyacrylamide Hydrogel for the Treatment of Knee Osteoarthritis Symptoms: A Retrospective Case Series. Clin Ortho Adv Res J: COARJ-100001.
Pai, A., Al-Singary, W., 2015. Durability, safety and efficacy of polyacrylamide hydrogel (Bulkamid®) in the management of stress and mixed urinary incontinence: three year follow up outcomes. Cent European J Urol 68, 428-433.
Pallua, N., Wolter, T.P., 2010. A 5-year assessment of safety and aesthetic results after facial soft-tissue augmentation with polyacrylamide hydrogel (Aquamid): a prospective multicenter study of 251 patients. Plast.Reconstr.Surg. 125, 1797-1804.
Petterson, S.C., Plancher, K.D., 2019. Single intra-articular injection of lightly cross-linked hyaluronic acid reduces knee pain in symptomatic knee osteoarthritis: a multicenter, double-blind, randomized, placebo-controlled trial. Knee surgery, sports traumatology, arthroscopy : official journal of the ESSKA 27, 1992-2002.
Phillips, M., Vannabouathong, C., Devji, T., Patel, R., Gomes, Z., Patel, A., Dixon, M., Bhandari, M., 2020. Differentiating factors of intra-articular injectables have a meaningful impact on knee osteoarthritis outcomes: a network meta-analysis. Knee surgery, sports traumatology, arthroscopy : official journal of the ESSKA 28, 3031-3039.
Price, A.J., Alvand, A., Troelsen, A., Katz, J.N., Hooper, G., Gray, A., Carr, A., Beard, D., 2018. Knee replacement. Lancet 392, 1672-1682.
Rauso, R., 2015. 5-year study of a polyacrylamide hydrogel-based filler for rehabilitation of HIV-related facial lipoatrophy. Aesthet Surg J 35, 1021-1029.
Rauso, R., Califano, L., Rugge, L., Chirico, F., Tartaro, G., 2018. Late Onset Complications Secondary to Polyacrylamide Hydrogel-Based Filler for Rehabilitation of HIV-Related Facial Lipoatropy. Aesthet Surg J 38, Np170-np174.
Rutjes, A.W., Juni, P., da Costa, B.R., Trelle, S., Nuesch, E., Reichenbach, S., 2012. Viscosupplementation for osteoarthritis of the knee: a systematic review and meta-analysis. Annals of internal medicine
157, 180-191.
Rydell, N., Butler, J., Balazs, E.A., 1970. Hyaluronic acid in synovial fluid. VI. Effect of intra-articular injection of hyaluronic acid on the clinical symptoms of arthritis in track horses. Acta veterinaria Scandinavica 11, 139-155.
Shen, D., Chen, M., Chen, K., Wang, T., Lu, L., Yang, X., 2018. Efficacy of hyaluronic acid after knee arthroscopy: A systematic review and meta-analysis. Journal of rehabilitation medicine 50, 860-865.
Siddiqui, Z.A., Abboudi, H., Crawford, R., Shah, S., 2017. Intraurethral bulking agents for the management of female stress urinary incontinence: a systematic review. Int Urogynecol J.
Skou, S.T., Roos, E.M., Laursen, M.B., Rathleff, M.S., Arendt-Nielsen, L., Rasmussen, S., Simonsen, O., 2018. Total knee replacement and non-surgical treatment of knee osteoarthritis: 2-year outcome from two parallel randomized controlled trials. Osteoarthritis and cartilage / OARS, Osteoarthritis Research Society 26, 1170-1180.
Skou, S.T., Roos, E.M., Laursen, M.B., Rathleff, M.S., Arendt-Nielsen, L., Simonsen, O., Rasmussen, S., 2015. A Randomized, Controlled Trial of Total Knee Replacement. The New England journal of medicine 373, 1597-1606.
Sokol, E.R., Karram, M.M., Dmochowski, R., 2014. Efficacy and safety of polyacrylamide hydrogel for the treatment of female stress incontinence: a randomized, prospective, multicenter North American study. J Urol 192, 843-849.
Steinhaus, M.E., Christ, A.B., Cross, M.B., 2017. Total Knee Arthroplasty for Knee Osteoarthritis: Support for a Foregone Conclusion? HSS journal : the musculoskeletal journal of Hospital for Special Surgery 13, 207-210.
Sun, S.F., Hsu, C.W., Lin, H.S., Liou, I.H., Chen, Y.H., Hung, C.L., 2017. Comparison of Single Intra-Articular Injection of Novel Hyaluronan (HYA-JOINT Plus) with Synvisc-One for Knee Osteoarthritis: A Randomized, Controlled, Double-Blind Trial of Efficacy and Safety. The Journal of bone and joint surgery. American volume 99, 462-471.
Tammachote, N., Kanitnate, S., Yakumpor, T., Panichkul, P., 2016. Intra-Articular, Single-Shot Hylan G-F 20 Hyaluronic Acid Injection Compared with Corticosteroid in Knee Osteoarthritis: A Double-Blind, Randomized Controlled Trial. The Journal of bone and joint surgery. American volume 98, 885-892.
Tnibar, A., Britt Persson, A., Elvang Jensen, H., 2017. Mechanisms of Action of an Intraarticular 2.5% Polyacrylamide Hydrogel (Arthramid Vet) in a Goat Model of Osteoarthritis: Preliminary Observations. SM Journal of Biomedical Engineering 3, 1022.
Tnibar, A., Persson, A.B., Nielsen, H., Svalastoga, E., Westrup, U., McEvoy, F., Knudsen, J., Thomsen, P.D., Berg, L.C., Jacobsen, S., Christensen, L.H., 2014a. Evaluation of a polyacrylamide hydrogel in the treatment of induced osteoarthritis in a goat model: a randomized controlled pilot study. Abs. 871. Osteoarthritis and Cartilage 22, S477.
Tnibar, A., Schougaard, H., Camitz, L., Rasmussen, J., Koene, M., Jahn, W., Markussen, B., 2015. An international multi-centre prospective study on the efficacy of an intraarticular polyacrylamide hydrogel in horses with osteoarthritis: a 24 months follow-up. Acta veterinaria Scandinavica 57, 20.
Tnibar, A., Schougaard, H., Koene, M., Christensen, L., Markussen, B., 2014b. A controlled clinical trial on the efficacy of an intra-articular Polyacrylamide Hydrogel in horses with osteoarthritis [abstract]. Veterinary Surgery 43, E138.
Tonbul, M., Adas, M., Bekmezci, T., Kara, A.D., 2014. Intra-articular polyacrylamide hydrogel injections are not innocent. Case reports in orthopedics 2014, 150709.
Toozs-Hobson, P., Al-Singary, W., Fynes, M., Tegerstedt, G., Lose, G., 2012. Two-year follow-up of an open-label multicenter study of polyacrylamide hydrogel (Bulkamid(R)) for female stress and stress-predominant mixed incontinence. Int. Urogynecol. J.
Trojian, T.H., Concoff, A.L., Joy, S.M., Hatzenbuehler, J.R., Saulsberry, W.J., Coleman, C.I., 2016. AMSSM scientific statement concerning viscosupplementation injections for knee osteoarthritis: importance for individual patient outcomes. British journal of sports medicine 50, 84-92.
Vallejo, A., Garcia-Ruano, A.A., Pinilla, C., Castellano, M., Deleyto, E., Perez-Cano, R., 2017. "Comparing efficacy and costs of four facial fillers in HIV-associated lipodystrophy: a clinical trial.". Plast Reconstr Surg.
Vecchioli-Scaldazza, C., 2014. Polyacrylamide hydrogel (Bulkamid®) in female patients of 80 or more years with urinary incontinence. Int Braz J Urol. 40, 37-43.
Wilson, M.G., Kelley, K., Thornhill, T.S., 1990. Infection as a complication of total knee-replacement arthroplasty. Risk factors and treatment in sixty-seven cases. The Journal of bone and joint surgery. American volume 72, 878-883.
Yan, C.H., Chan, W.L., Yuen, W.H., Yung, P.S., Ip, K.Y., Fan, J.C., Chiu, K.Y., 2015. Efficacy and safety of hylan G-F 20 injection in treatment of knee osteoarthritis in Chinese patients: results of a prospective, multicentre, longitudinal study. Hong Kong medical journal = Xianggang yi xue za zhi 21, 327-332.
Zar, V.V., Zagorodniy, N.V., Martinov, D.V., 2012. Effectiveness and safety of injectable endprosthetics of sinovial fluid by cross-linked polimer Noltrex for treatment OA knee. European Journal of Musculoskeletal Diseases 1, 23-32.
Zarini, E., Supino, R., Pratesi, G., Laccabue, D., Tortoreto, M., Scanziani, E., Ghisleni, G., Paltrinieri, S., Tunesi, G., Nava, M., 2004. Biocompatibility and tissue interactions of a new filler material for medical use. Plast.Reconstr.Surg. 114, 934-942.
Zhao, H., Liu, H., Liang, X., Li, Y., Wang, J., Liu, C., 2016. Hylan G-F 20 Versus Low Molecular Weight Hyaluronic Acids for Knee Osteoarthritis: A Meta-Analysis. BioDrugs : clinical immunotherapeutics, biopharmaceuticals and gene therapy 30, 387-396.
Zivanovic, I., Rautenberg, O., Lobodasch, K., von Bunau, G., Walser, C., Viereck, V., 2017. Urethral bulking for recurrent stress urinary incontinence after midurethral sling failure. Neurourol Urodyn 36, 722-726.